
The SR1 form is a UK medical report used to support fast-tracked benefit claims for people with a terminal illness. A doctor or specialist completes the form to confirm that a patient has a progressive condition and may not live beyond 12 months.
The SR1 form replaced the DS1500 form, allowing eligible individuals to access higher-rate benefits more quickly without a medical assessment.
Key Takeaways
- The SR1 form UK is used to fast-track benefit claims under special rules for terminal illness
- It replaces the older DS1500 form (also known as DS1500)
- A healthcare professional must complete the form; patients cannot fill it themselves
- Claims supported by an SR1 form are processed faster and often qualify for higher payments
- No face-to-face medical assessment is required in most cases
For care providers, understanding what is an SR1 form is essential. It helps you guide families through urgent financial support options and ensures clients receive the care they need without delays.
Why the SR1 Form Matters for Care Providers
Care providers play a critical role in identifying when a client may need an SR1 form. Acting early can significantly improve a client’s access to financial support and ensure continuity of care during a difficult time.
When a client qualifies under the special rules, the sr1 form allows them to receive benefits quickly—often at the highest rate. This means families can afford consistent care services, whether that involves domiciliary care, specialist support, or additional staffing needs.
How the SR1 Form Supports Better Care Outcomes
- Faster funding decisions: Clients receive financial support within days instead of weeks
- Improved care planning: Providers can deliver services without delays caused by financial uncertainty
- Reduced stress for families: Families focus on care and emotional support instead of complex benefit processes
- Higher likelihood of sustained care packages: Access to enhanced benefit rates helps maintain long-term care arrangements
Your Role as a Care Provider
Care providers often notice changes in a client’s condition before anyone else. You can:
- Recognise when a condition becomes life-limiting
- Encourage families to speak with a GP or specialist
- Ensure the sr1 process starts early to avoid delays in support
The earlier a care provider flags the need for an SR1 form, the faster a client can access the financial support required to maintain quality care.
By understanding what is an SR1 form and when to use it, care providers position themselves as trusted partners in both care delivery and client advocacy.
RELATED: What is the Health and Safety at Work Act 1974?
What is an SR1 Form and How Does It Work?
An SR1 form is a medical report completed by a healthcare professional to confirm that a patient has a progressive, life-limiting condition. It allows the Department for Work and Pensions (DWP) to process benefit claims under the special rules for terminal illness, without requiring a full medical assessment.
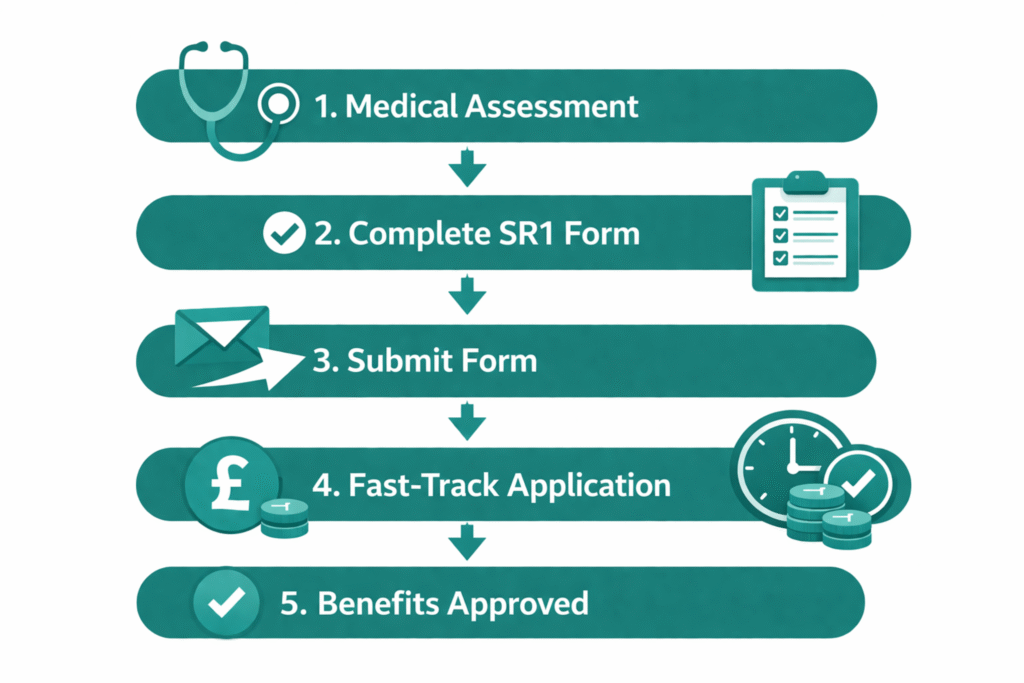
How the SR1 Process Works (Step-by-Step)
- A clinician identifies eligibility
A GP, consultant, or specialist nurse determines that the patient has a progressive condition and may not live beyond 12 months.
- The healthcare professional completes the SR1 form
The clinician records key medical details, including diagnosis, progression, and clinical indicators.
- The SR1 form is submitted to the DWP
The form is usually sent directly by the clinician via secure systems or email.
- The patient applies for benefits under special rules
The claim must clearly state that it is being made under the special rules for terminal illness.
- The claim is fast-tracked and prioritised
Applications supported by an SR1 are processed quickly and often awarded at the highest rate.
Key Things to Know About How It Works
- The sr1 form uk does not require a detailed life expectancy—clinicians use their professional judgment
- The process focuses on speed, reducing delays in accessing support
- The patient does not need to attend a medical assessment in most cases
The sr1 form acts as trusted medical evidence, allowing benefit decisions to be made quickly and with minimal stress for the patient and their family.
For care providers, understanding what is sr1 form and how it works helps you guide families through a time-sensitive process and ensures no unnecessary delays in securing essential support.
SR1 Form vs DS1500 Form: What Changed?
The SR1 form replaced the older DS1500 form to improve how people with terminal illnesses access benefits in the UK. While both forms serve the same purpose, supporting fast-tracked claims, the SR1 introduces a more modern, flexible, and clinician-friendly approach.
Key Differences Between SR1 and DS1500
| Feature | SR1 Form | DS1500 Form |
| Status | Current system | Replaced (legacy) |
| Purpose | Fast-track benefit claims | Same purpose |
| Prognosis requirement | No strict timeline wording required | Previously more rigid |
| Submission | Digital, email, or post | Mostly paper-based |
| Clinician experience | Simplified and more flexible | More formal and restrictive |
- Improved access to support: The SR1 form makes it easier for clinicians to confirm eligibility without rigid wording
- Faster processing: Digital submission options reduce delays compared to the ds1500 form
- Better clinical judgment: Doctors can use professional discretion instead of fixed criteria
The transition from the DS1500 form to the SR1 form UK reflects a shift toward faster, more compassionate support for people with life-limiting conditions.
What Care Providers Should Know
- Some families and even professionals may still refer to the ds1500, but it is no longer the standard
- Always guide clients toward the sr1 form when applying under special rules
- Understanding this change helps you avoid confusion and ensures the correct process is followed
By clearly explaining the difference between the SR1 form and the DS1500 form, care providers can support families more effectively and prevent delays in accessing critical benefits.
READ MORE: How Much Is JSA (Jobseeker’s Allowance) in 2026?
Who Qualifies for an SR1 Form?
A patient qualifies for an SR1 form if they have a progressive, life-limiting condition, and a clinician would not be surprised if they were to live for less than 12 months. This definition focuses on clinical judgment rather than a strict prognosis, making the SR1 form UK more flexible and easier to apply in practice.
Core Eligibility Criteria
To qualify for an sr1 form, the patient must:
- Have a progressive disease (the condition is worsening over time)
- Be considered life-limiting by a healthcare professional
- Meet the clinical threshold where a doctor would not be surprised if death occurs within 12 months
Conditions That May Qualify
The SR1 form is not limited to cancer. Patients with a wide range of conditions may qualify, including:
- Advanced cancer
- Organ failure (heart, lung, liver, kidney)
- Neurological conditions (e.g. motor neurone disease, multiple sclerosis)
- Advanced dementia
- Severe frailty or complex comorbidities
Eligibility for an SR1 depends on the overall clinical picture, not just a specific diagnosis.
Important Clarifications
- A patient does not need to be in their final days or weeks to qualify
- Clinicians do not need to provide an exact life expectancy
- If a patient lives longer than expected, there are no penalties for the clinician or the patient
Why This Matters for Care Providers
Care providers often see early signs of decline before a formal diagnosis reaches its final stage. You can:
- Identify when a client’s condition becomes significantly progressive
- Prompt timely conversations with healthcare professionals
- Help families understand when an SR1 form may be appropriate
Recognizing eligibility early ensures clients receive financial support without unnecessary delays.
By understanding what is a SR1 form and who qualifies, care providers can act quickly and play a key role in securing timely support for vulnerable clients.
Who Can Complete an SR1 Form?
Only qualified healthcare professionals can complete an SR1 form. This ensures that the medical evidence used to fast-track benefit claims is accurate, credible, and accepted by the Department for Work and Pensions (DWP).
Healthcare Professionals Who Can Complete an SR1 Form
The following professionals can complete and submit an sr1 form:
- General Practitioners (GPs)
- Hospital consultants
- Hospice doctors
- Specialist or advanced nurse practitioners (e.g. clinical nurse specialists, Macmillan nurses)
- Other registered clinicians with relevant expertise
The clinician must have sufficient knowledge of the patient’s condition to make an informed clinical judgment.
Who Cannot Complete an SR1 Form
- Patients themselves
- Family members or caregivers
- Non-clinical staff
The sr1 form must always come from a recognised medical professional to be valid.
How Care Providers Should Work With Clinicians
Care providers do not complete the SR1 form, but they play an important supporting role:
- Raise concerns early: Flag changes in a client’s condition to the GP or care team
- Encourage timely action: Prompt families to request an SR1 when appropriate
- Support communication: Share relevant observations that may help clinicians assess eligibility
Delays often happen because no one initiates the conversation with a clinician. Care providers are in a strong position to bridge that gap.
When care providers collaborate effectively with healthcare professionals, the SR1 form process starts earlier, helping clients access urgent financial support without delay.
Understanding who can complete an SR1 form UK helps you guide families correctly and ensures the process runs smoothly from the start.
SEE ALSO: What Is an Enhanced DBS CRB Check? 2026 Update for Care Homes
How to Get an SR1 Form (Step-by-Step)
You cannot download or request an SR1 form yourself. A healthcare professional must issue and complete it on your behalf. As a care provider, you can guide families through the correct steps to avoid delays.
Step-by-Step: How to Get an SR1 Form
- Identify when the SR1 may be needed
Recognise signs of a progressive, life-limiting condition and raise this with the care team.
- Speak to a healthcare professional
Ask the client’s GP, hospital consultant, or specialist nurse about completing an sr1 form.
- Clinician assesses eligibility
The healthcare professional uses their judgment to decide if the patient meets the criteria.
- The SR1 form is completed by the clinician
The clinician records diagnosis, progression, and relevant clinical details.
- The form is submitted to the DWP
In most cases, the clinician sends the sr1 form directly.
Can You Download an SR1 Form?
- The SR1 form download is not available to the public
- Patients and families cannot access or complete the form themselves
- Only authorised clinicians can request or generate the form
If a family asks for an SR1 form printable version, guide them to their GP or specialist instead of searching online.
How Care Providers Can Speed Up the Process
- Act early when a client’s condition declines
- Encourage families to request an SR1 during medical reviews
- Follow up with clinicians if delays occur
The fastest way to secure an SR1 form UK is through direct communication with the patient’s healthcare team.
By understanding how to get an SR1 form, care providers can remove confusion, prevent unnecessary delays, and ensure clients access financial support as quickly as possible.
Can You Complete the SR1 Form Online?
Healthcare professionals can complete and submit the SR1 form online, but patients and families cannot access or fill it out themselves. The digital process is designed to speed up submissions and ensure secure handling of medical information.
How the SR1 Form Online Process Works
- Clinicians request or access the form through secure NHS systems
- They complete the SR1 form online using clinical details and professional judgment
- The form is submitted directly to the Department for Work and Pensions (DWP) via secure channels
In many cases, digital submission replaces the need for postal forms, reducing delays and improving processing times.
NHS Systems Used for Submission
Healthcare professionals may use secure platforms such as:
- NHS Spine (nhsspine)
- NHS smartcard portal for authentication
- Secure NHS email systems
These systems ensure that sensitive patient data is transmitted safely and efficiently.
The use of secure systems like the nhs spine allows clinicians to submit the SR1 form quickly, helping patients access urgent financial support without unnecessary delays.
What This Means for Care Providers
- You do not need to handle or submit the form yourself
- Your role is to ensure the right conversation happens with the clinician
- Digital submission means faster turnaround for your clients
Encouraging clinicians to use the SR1 form online process can significantly reduce waiting times for benefit approvals.
Is There an SR1 Form Printable Version?
- A sr1 form printable version exists for clinicians, but it is not publicly accessible
- Most submissions now happen digitally due to speed and security advantages
By understanding how the SR1 form online process works, care providers can better support families and ensure no time is lost when urgent financial help is needed.
MORE: Central Reservations System for Caregivers UK: Importance of Digital Care Management
What Benefits Can an SR1 Form Unlock?
An SR1 form allows patients with a terminal illness to access certain UK benefits under special rules. These claims are prioritized, processed faster, and often awarded at the highest rate, making them essential for maintaining consistent care and financial stability.
Benefits That Accept an SR1 Form
A completed sr1 form UK can support fast-tracked claims for:
- Personal Independence Payment (PIP)
- Universal Credit (UC)
- Employment and Support Allowance (ESA)
- Disability Living Allowance (DLA) (for children)
- Attendance Allowance (AA)
The sr1 form acts as medical evidence that allows these benefits to be processed under special rules for terminal illness.
What Changes When an SR1 Form Is Used
When a claim includes an SR1 form, the process becomes significantly easier:
- No medical assessment required in most cases
- Faster decision-making, often within days
- Higher rate of payment, depending on the benefit
Why This Matters for Care Providers
Access to these benefits directly affects the level and continuity of care a client can receive. With faster approvals:
- Clients can afford immediate care support
- Families can reduce financial pressure during critical periods
- Care providers can deliver consistent and uninterrupted services
The SR1 form bridges the gap between urgent care needs and financial support, ensuring that vulnerable clients receive help when it matters most.
Key Insight for Care Teams
Many families are unaware that these benefits can be fast-tracked. Care providers who understand what is an SR1 form can:
- Educate families about available support
- Encourage early application under special rules
- Prevent delays that could impact care delivery
By knowing which benefits the SR1 form unlocks, care providers can play a proactive role in securing timely support for their clients.
Key Benefits of Using an SR1 Form
Using an SR1 form transforms how quickly and easily a patient can access financial support. For care providers, this directly impacts how fast care plans can be implemented and sustained.
1. No Medical Assessment Required
Patients supported by an sr1 form usually do not need to attend a face-to-face medical assessment. This removes delays and avoids unnecessary stress for individuals in a vulnerable condition.
2. Fast-Tracked Processing
Claims submitted with an SR1 form UK are prioritised by the Department for Work and Pensions (DWP).
- Decisions are often made within days, not weeks
- Urgent financial support becomes available much sooner
The sr1 form ensures that time-sensitive cases receive immediate attention.
3. Higher Rate of Payments
Most claims supported by an SR1 form qualify for the enhanced or highest rate of benefits.
This allows patients to:
- Cover increased care costs
- Access specialist support
- Maintain quality of life
4. Reduced Administrative Burden
The sr1 simplifies the claims process:
- Less paperwork compared to standard applications
- Fewer follow-ups required
- Minimal back-and-forth with assessors
Why This Matters for Care Providers
When a client uses an SR1 form, everything moves faster:
- Care packages can start immediately
- Funding gaps are reduced
- Families gain peace of mind
The SR1 form is not just a document; it is a critical tool that enables timely care, financial stability, and better outcomes for patients and their families.
Understanding these benefits allows care providers to act quickly and ensure no client misses out on essential support.
READ: Children’s DLA Rates: Who Qualifies, and What to Claim in 2026
When Should Care Providers Request an SR1 Form?
Care providers should raise the need for an SR1 form as soon as a client shows signs of a progressive, life-limiting condition. Acting early ensures the client can access fast-tracked financial support without delays.
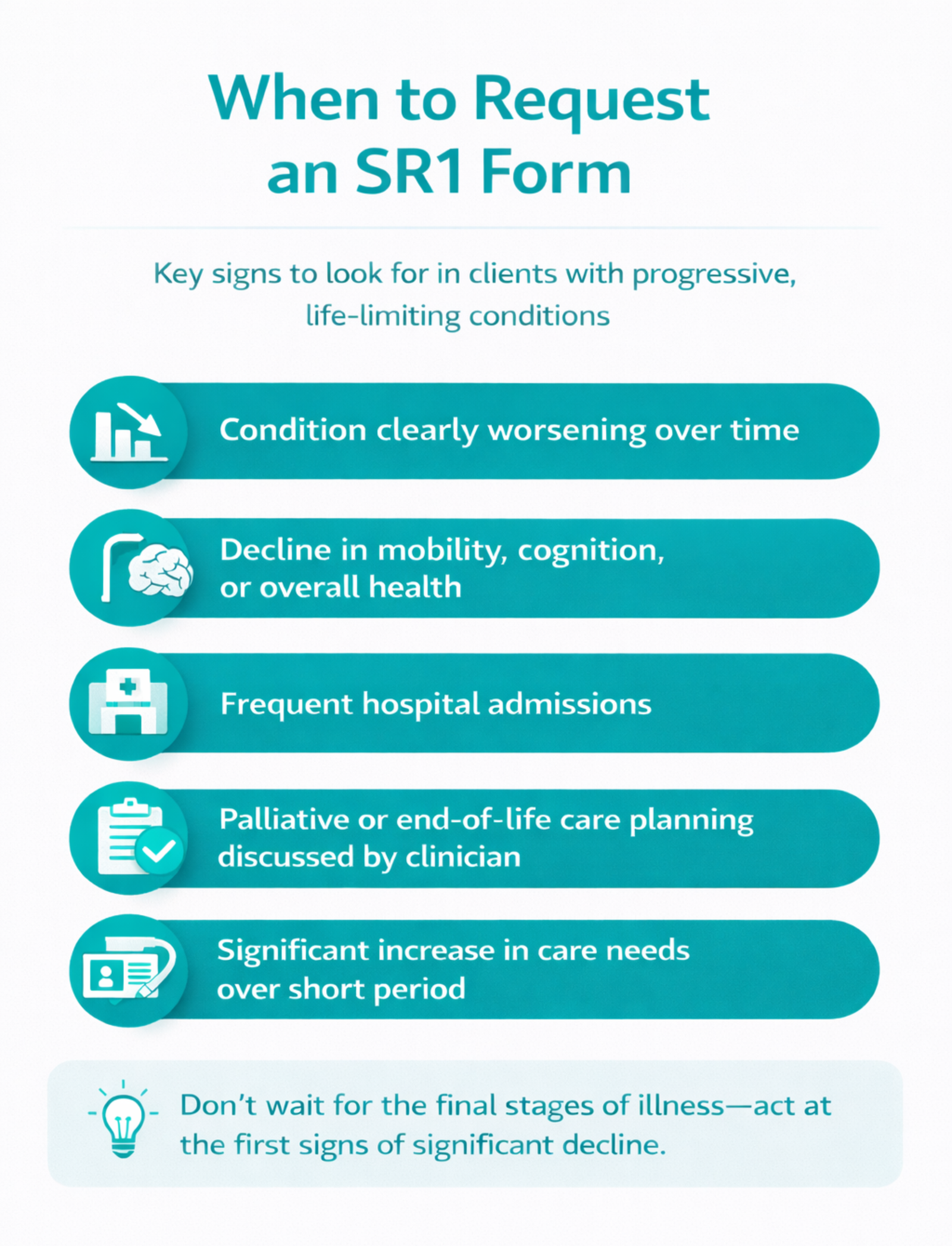
Key Moments to Consider an SR1 Form
You should prompt a conversation about the sr1 form when:
- A client’s condition is clearly worsening over time
- There is a noticeable decline in mobility, cognition, or overall health
- Hospital admissions become more frequent
- A clinician discusses palliative or end-of-life care planning
- Care needs increase significantly within a short period
Do not wait for the final stages of illness. The SR1 form applies earlier than many people realise.
Why Timing Matters
Delaying the sr1 form UK process can lead to:
- Gaps in funding for care services
- Increased stress for families
- Delayed access to enhanced benefits
Starting early allows:
- Faster approvals
- Smoother care planning
- Better support for both clients and families
How Care Providers Can Take Action
- Observe and document changes in the client’s condition
- Communicate concerns to the GP or care team promptly
- Encourage families to request an SR1 during medical reviews
- Follow up if the process is delayed
Expert Insight
Care providers often spend the most time with clients. Your observations can trigger the SR1 form process at the right time, ensuring clients receive the support they need without unnecessary waiting.
By recognising the right moment to request an SR1 form, care providers can take a proactive role in improving outcomes and ensuring timely access to essential benefits.
Common Mistakes Care Providers Should Avoid
Even when care providers understand the SR1 form, small mistakes can delay access to urgent financial support. Avoiding these errors ensures clients receive benefits quickly and without complications.
1. Waiting Too Long to Raise the SR1 Form
Many providers assume the sr1 form only applies in the final days or weeks of life. This is incorrect.
- The criteria focus on a progressive condition, not exact timing
- Delaying the conversation can slow down access to benefits
Raise the possibility of an SR1 form as soon as a client’s condition shows significant decline.
2. Assuming Only Cancer Patients Qualify
The SR1 form UK applies to a wide range of conditions, including:
- Organ failure
- Neurological diseases
- Advanced dementia
- Complex frailty
Limiting it to cancer cases prevents eligible clients from receiving support.
3. Not Communicating with Clinicians Early
Care providers often notice changes first, but delays happen when:
- No one informs the GP or specialist
- Families are unsure how to start the process
Early communication with healthcare professionals speeds up the sr1 process significantly.
4. Expecting Families to Handle Everything Alone
Families may not understand:
- What an SR1 form is
- How to request it
- Why it matters
Care providers should guide them clearly and confidently.
5. Misunderstanding the Process
Common misconceptions include:
- Believing patients can complete the sr1 form themselves
- Thinking a formal prognosis is required
- Assuming there are penalties if a patient lives longer than expected
These misunderstandings can create unnecessary delays or hesitation.
Why Avoiding These Mistakes Matters
Mistakes in the SR1 form process can:
- Delay benefit approvals
- Interrupt care services
- Increase stress for families
Getting the SR1 form process right the first time ensures clients receive fast, reliable support when they need it most.
By avoiding these common pitfalls, care providers strengthen their role as trusted advisors and improve outcomes for the people they support.
ALSO SEE: NHS Hearing Aids UK: Cost, Types, Waiting Times, and How to Get One in 2026
SR1 Form Example: What Information Is Required?
An SR1 form is a clinical document, not a detailed medical report. It focuses on key information that allows the Department for Work and Pensions (DWP) to quickly confirm eligibility under special rules.
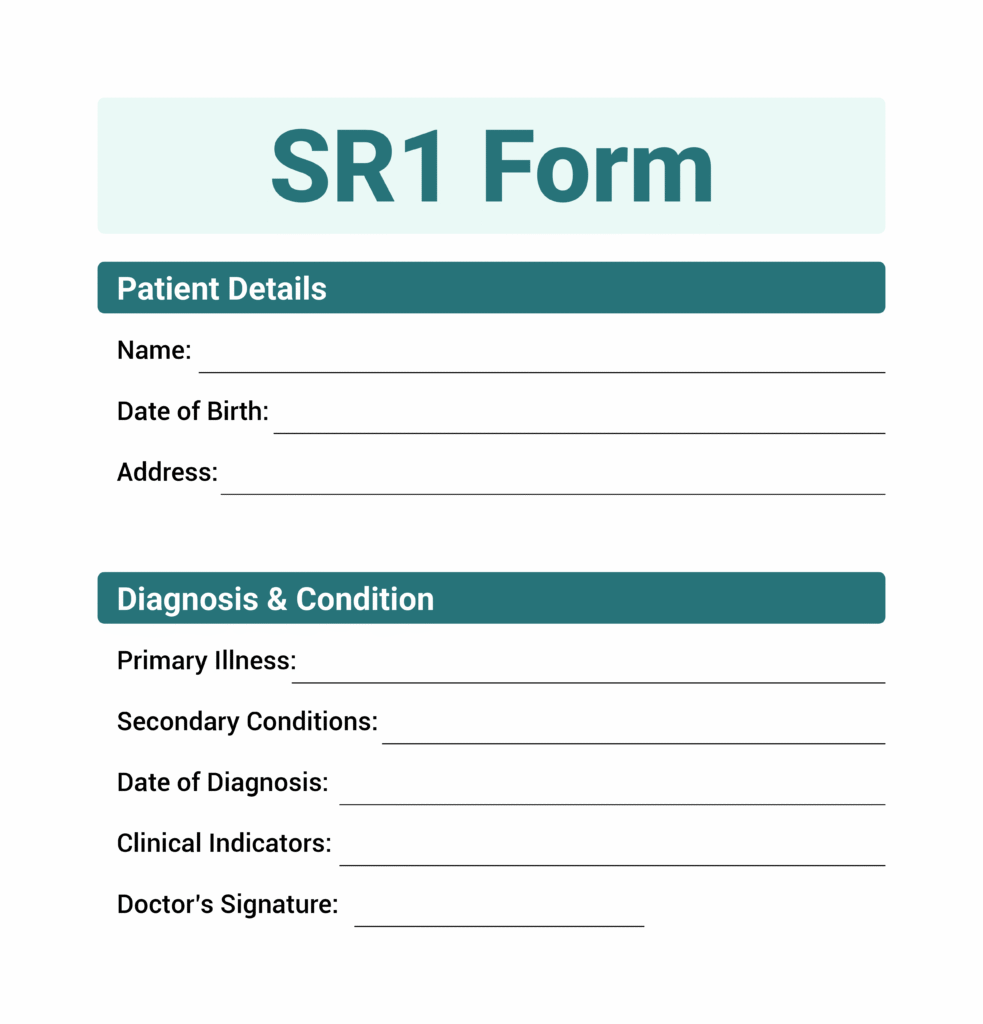
SR1 Form Example: Core Information Included
A typical sr1 form example will include:
- Patient details
Name, date of birth, and address
- Diagnosis and condition
Primary illness and any relevant secondary conditions
- Date of diagnosis
When the condition was first identified
- Clinical indicators
Evidence that the condition is progressive and life-limiting
- Awareness of condition
Whether the patient understands their diagnosis and prognosis
- Treatment plan
Current or planned care approach
- Clinician details
Name, role, registration number, and organisation
How Clinicians Complete the SR1 Form
Healthcare professionals complete the SR1 form using clear clinical language. They do not need to:
- Provide an exact life expectancy
- Write lengthy explanations
- Include unnecessary medical history
The goal of the sr1 form is to confirm eligibility quickly, not to produce a full medical assessment.
What Care Providers Should Know
Care providers do not complete the SR1 form, but understanding its structure helps you:
- Explain the process confidently to families
- Prepare relevant information for discussions with clinicians
- Ensure nothing delays submission
Important Note
- There is no publicly available SR1 form printable or editable version for patients
- Only authorised clinicians can access and complete the official form
Understanding a basic SR1 form example helps care providers support the process more effectively and avoid confusion.
By knowing what information the SR1 form requires, care providers can play a proactive role in ensuring timely and accurate submissions.
Final Thoughts…
The SR1 form is one of the most important tools available to support clients with life-limiting conditions. It enables fast access to financial support, removes unnecessary assessments, and ensures care can continue without interruption.
As a care provider, you are often the first to recognise when a client’s condition is declining. Acting on that insight, by encouraging an SR1 form request at the right time, can make a significant difference to both the client and their family.
What Care Providers Should Remember
- Act early when a condition becomes progressive
- Guide families clearly through the SR1 form UK process
- Communicate effectively with healthcare professionals
- Avoid delays by addressing eligibility as soon as possible
The SR1 form is not just paperwork; it is a gateway to timely support, dignity, and better care outcomes.
By understanding what is an SR1 form and using that knowledge in practice, care providers position themselves as trusted partners in both care delivery and client advocacy.
Need Help Navigating SR1 Forms and Care Compliance?
At Care Sync Experts, we support care providers in handling critical processes like the SR1 form with clarity, speed, and confidence.
Whether you need help with:
- Understanding when to request an SR1 form for your clients
- Supporting families through fast-tracked benefit applications
- Ensuring compliance with CQC and care regulations
- Strengthening your care operations and documentation
- Preparing your business for growth, contracts, and inspections
We’re here to guide you every step of the way.
Don’t let delays in the SR1 form UK process affect your clients’ access to essential support.
Let our experts simplify the process so you can focus on delivering high-quality care.
Get Started Today
Book a consultation with Care Sync Experts and ensure your care business is equipped to support clients when it matters most.
FAQ
What is a S1 form in the UK?
The S1 form is different from the SR1 form. It is used for healthcare access, not benefits. An S1 form allows UK nationals living in another European country (or vice versa) to access state healthcare funded by the UK. It has no connection to terminal illness benefit claims.
How much is terminal illness benefit in the UK?
There is no single “terminal illness benefit.” Instead, individuals receive fast-tracked access to existing benefits (such as PIP, UC, ESA, or Attendance Allowance). In most cases, claims supported under special rules qualify for the highest rate, which can range from around £72 to over £180 per week depending on the benefit.
How do I apply for Attendance Allowance in England?
To apply for Attendance Allowance, you must:
– Request or download the claim form from GOV.UK or by phone
– Complete the form with details about care needs
– Indicate if you are applying under special rules for terminal illness
– Ask a healthcare professional to complete an SR1 form
– Submit the application by post
Claims supported by an SR1 form are processed faster and usually awarded at the higher rate.
How much is full Attendance Allowance in the UK?
As of current UK rates, the higher rate of Attendance Allowance is approximately £108.55 per week (subject to annual updates). People who apply under special rules for terminal illness are typically awarded this higher rate automatically.







{kind=link}