The 5 principles of Mental Capacity Act guide how caregivers, families, and care providers support people who may struggle to make certain decisions. These principles come from the Mental Capacity Act 2005, which applies in England and Wales and protects people aged 16 and over.
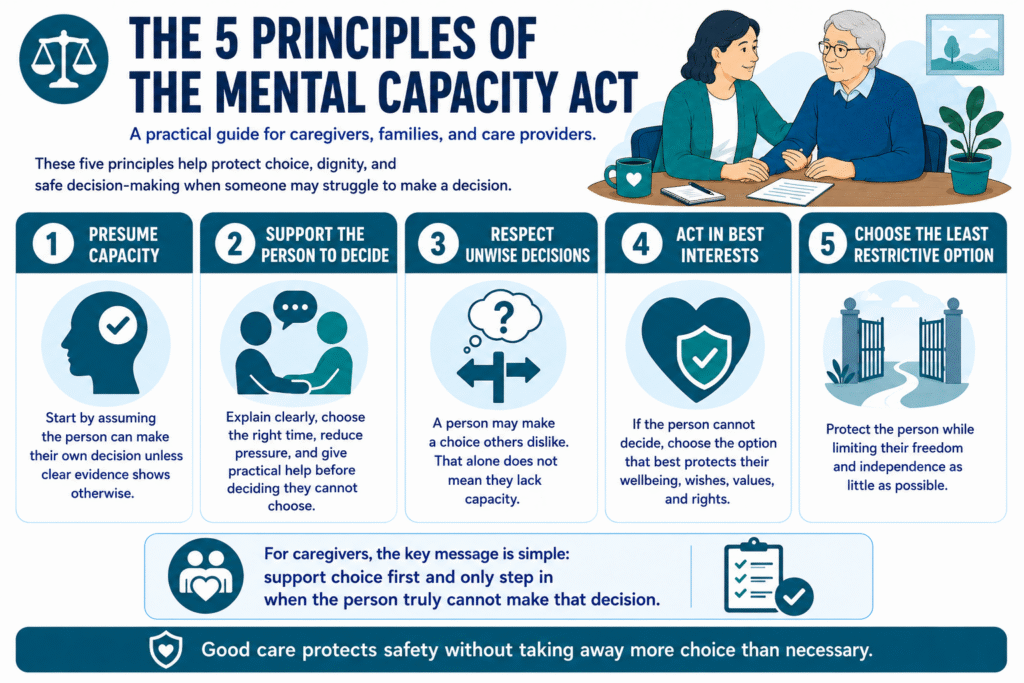
The five principles are simple but powerful: presume the person has capacity, support them to make their own decision, respect their right to make an unwise decision, act in their best interests if they lack capacity, and choose the least restrictive option.
For caregivers, the message is clear: do not take over too quickly. A person may need time, reassurance, simpler information, or a better way to communicate before they can decide.
Good care starts by protecting choice. Before a care worker makes or supports a decision, they should ask: Can this person decide with the right support? That question sits at the heart of safe, respectful, person-centred care.
What Is the Mental Capacity Act?
The Mental Capacity Act 2005 is a law that protects people who may not be able to make a specific decision for themselves. It also guides caregivers, families, health professionals, and care providers on how to support decisions safely and respectfully.
So, what does MCA stand for? MCA stands for Mental Capacity Act.
A simple Mental Capacity Act 2005 summary is this: the law helps people make their own decisions wherever possible. When someone cannot make a specific decision, the law tells caregivers and professionals how to act in that person’s best interests while protecting their rights and freedom.
In daily care, the MCA can apply to decisions about personal care, medication, meals, clothing, going out, managing money, hospital appointments, care visits, or moving into a care home.
The Act does not tell caregivers to control people. It tells them to support choice first, assess capacity properly, and only step in when the person truly cannot make that decision.
RELATED: What Is Respite Care in the UK? 2026
What Is Mental Capacity?
Mental capacity means a person can make a specific decision at the time they need to make it. It is not about age, diagnosis, disability, or how someone looks. It is about whether the person can understand the decision, think through the information, and communicate what they want.
Capacity can change from one decision to another. A person may choose what to wear, what to eat, or when to go to bed, but still struggle with a bigger decision such as managing money, refusing care, or moving into a care home.
Capacity can also change during the day. Someone may feel confused in the evening but clearer in the morning. Another person may decide better when a caregiver explains things slowly, uses pictures, gives them time, or removes pressure.
For caregivers, this matters because you should not say, “They lack capacity” in a general way. You should ask, “Can this person make this decision, at this time, with the right support?”
Who Does the Mental Capacity Act Apply To?
The Mental Capacity Act applies to people aged 16 and over in England and Wales who may lack capacity to make a specific decision. It also applies to anyone who supports or makes decisions for that person, including care workers, nurses, doctors, social workers, family members, attorneys, and care providers.
So, who does the Mental Capacity Act 2005 protect? It protects people who may struggle to make decisions because of dementia, learning disabilities, brain injury, mental health conditions, stroke, serious illness, confusion, unconsciousness, or another impairment affecting the mind or brain.
Caregivers must not assume someone lacks capacity because they are elderly, disabled, distressed, forgetful, or living with a diagnosis. The law expects workers to start with respect: assume the person can decide unless an assessment shows otherwise.
In practice, who does the MCA apply to? It applies whenever a caregiver supports a person who may not understand, retain, weigh up, or communicate a decision at the time it needs to happen.
READ MORE: Universal Credit Compensation DWP: Can You Claim Money Back in 2026?
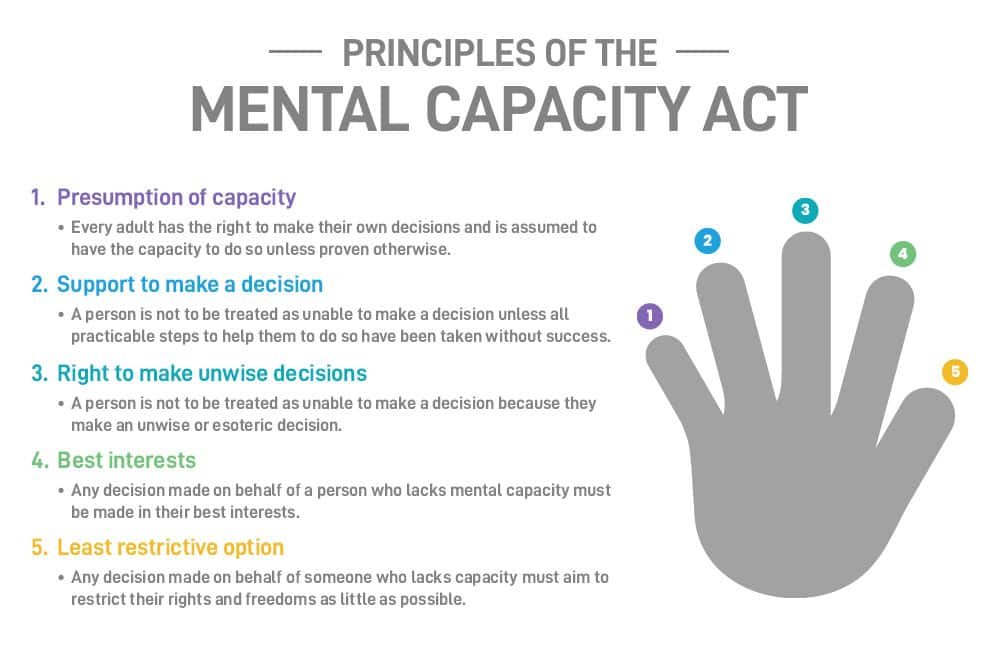
The 5 Principles of the Mental Capacity Act
There are five statutory principles within the MCA. Every caregiver should understand them because they shape how care workers support choice, safety, dignity, and rights.
1. Presume capacity
Start by assuming the person can make their own decision. Do not decide they lack capacity because of age, dementia, disability, appearance, or behaviour. Always begin with the belief that the person can decide unless there is clear evidence they cannot.
2. Support the person to decide
Before you say someone cannot decide, give them practical support. Use simple words, pictures, familiar routines, quiet spaces, or a trusted person. Choose the best time of day and give the person enough time to respond.
3. Respect unwise decisions
A person can make a choice that others see as unwise. That alone does not mean they lack capacity. Caregivers should focus on how the person makes the decision, not whether they personally agree with it.
4. Act in best interests
If the person cannot make the decision, workers must act in their best interests. This means considering their wishes, beliefs, values, safety, wellbeing, family input, and what they would likely choose if they could decide.
5. Choose the least restrictive option
When someone lacks capacity, choose the option that protects them while limiting their freedom as little as possible. Good care should reduce risk without taking away more control than necessary.
So, how many core principles are in the Mental Capacity Act? There are five. These 5 principles of Mental Capacity Act remind caregivers to support choice first and only step in when the person truly cannot decide.
How Do You Assess Mental Capacity?
Assessing mental capacity means checking whether a person can make a specific decision at the time the decision needs to happen. Caregivers should never assess capacity in a general way. They should focus on one decision at a time.
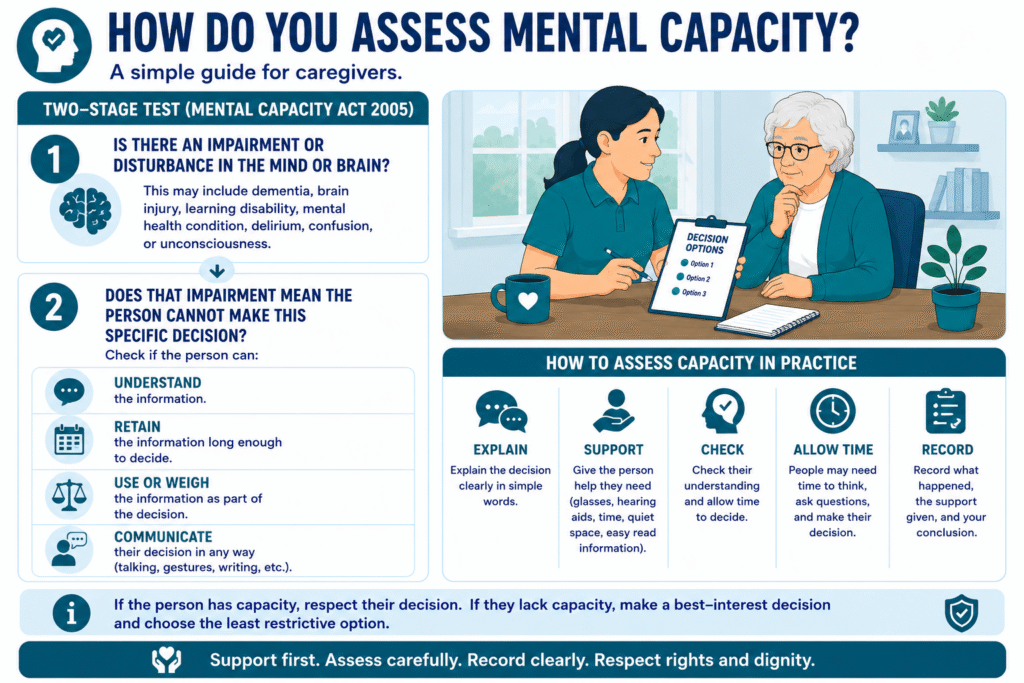
The Mental Capacity Act uses a two-stage test. First, ask whether the person has an impairment or disturbance in the mind or brain. This may include dementia, brain injury, learning disability, mental health condition, delirium, confusion, or unconsciousness.
Second, ask whether that impairment means the person cannot make the specific decision. To decide this, check whether the person can:
- Understand the information
- Retain the information long enough to decide
- Use or weigh the information
- Communicate their decision in any way
So, how do you assess mental capacity in care? You explain the decision clearly, give the person support, check their understanding, allow time, and record what happened.
Good caregivers do not rush this process. They support first, assess carefully, and document the reason for any decision made on the person’s behalf.
SEE ALSO: Band C Council Tax Per Month: What You Should Know in 2026
Who Can Assess Capacity and Make a Decision?
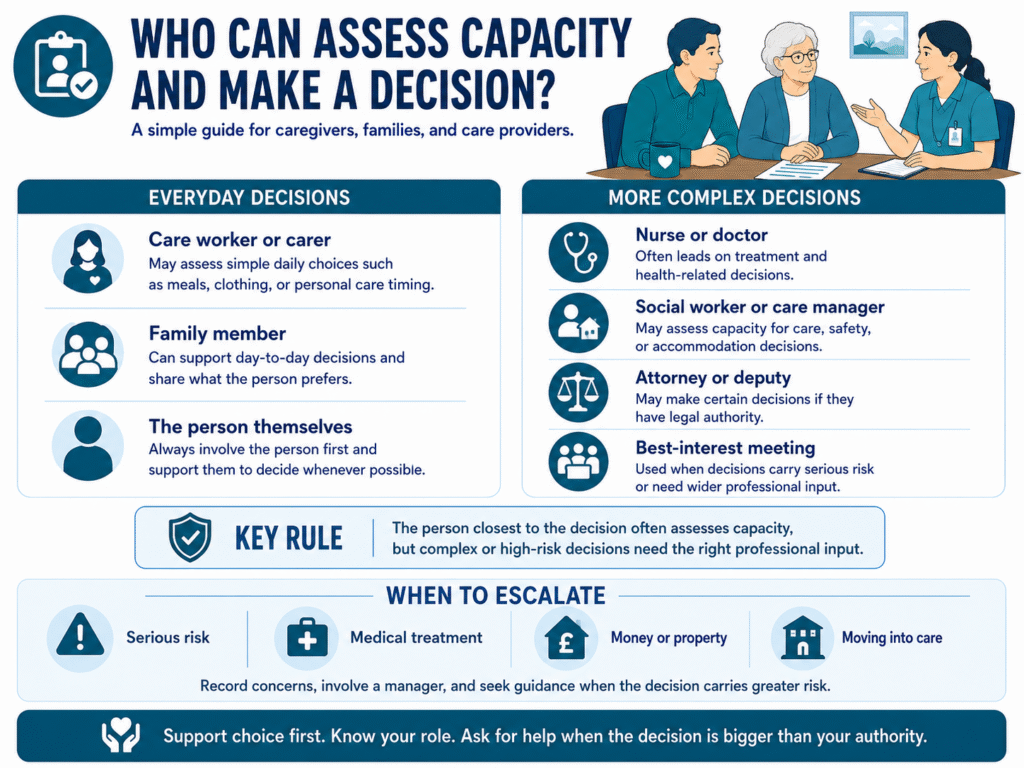
The person who needs the decision made usually assesses capacity for that decision. In daily care, this may be a care worker, nurse, care manager, social worker, doctor, or family member, depending on the type of decision.
For simple everyday choices, such as what to wear, what to eat, or whether to have a shower now or later, a care worker may assess whether the person can decide. For more serious decisions, such as medical treatment, moving into a care home, managing money, or refusing important care, the right professional should take the lead.
So, who can assess capacity and make a decision? The answer depends on the decision. The person closest to the decision should assess capacity, but complex or high-risk decisions often need senior staff, health professionals, social workers, attorneys, deputies, or a best-interest meeting.
Caregivers should know their limits. If a decision carries serious risk, they should record concerns, involve a manager, and seek professional guidance before acting.
When Must a Care Worker Comply With the Mental Capacity Act 2005?
A care worker must comply with the Mental Capacity Act 2005 whenever they support or make a decision for someone aged 16 or over who may lack capacity for that specific decision.
This can happen during ordinary care. For example, a person may refuse personal care, decline medication, choose unsafe food, want to go outside alone, reject care visits, or disagree with moving into a care home. In each situation, the worker must ask whether the person can understand the decision, weigh the risks, and communicate their choice.
To describe when a worker must comply with the Mental Capacity Act 2005, keep it simple: comply whenever a person’s ability to decide may be affected by dementia, brain injury, learning disability, mental health condition, confusion, illness, or another impairment of the mind or brain.
Care workers should not force support because they feel worried. They should explain, encourage, assess, record, and involve a manager or professional when risk increases. The MCA protects the person’s rights while guiding workers to act safely and lawfully.
MORE: Income Taxation UK: A Simple Guide for Care Businesses (2026)
What Does DoLS Allow You to Do?
DoLS means Deprivation of Liberty Safeguards. It applies when a person in a hospital or care home lacks capacity to agree to care arrangements that may restrict their freedom.
So, what does a DoLS allow you to do? It gives a legal framework for providing necessary care when restrictions protect the person from harm. For example, staff may need to supervise the person closely, stop them from leaving unsafely, or keep them in a care setting because they cannot understand the risks.
However, DoLS does not give care providers permission to ignore someone’s rights. It requires proper assessment, clear reasons, best-interest decision-making, and regular review.
From a caregiver’s perspective, DoLS should never feel like “control first.” Workers should still talk to the person, involve them as much as possible, respect their wishes, and choose the least restrictive option.
Good care protects safety without removing more freedom than necessary.
Final Thoughts…
The 5 principles of Mental Capacity Act do not ask caregivers to take control away from people. They ask caregivers to protect choice for as long as possible.
Good care starts with listening. Before you decide that someone cannot make a decision, explain the options clearly, reduce pressure, give them time, and check whether the right support could help them decide.
Families and care workers should also remember this: mental capacity can change. A person may struggle today but decide more clearly tomorrow. They may refuse care in the morning but accept it later when they feel calmer or when a trusted caregiver explains it differently.
When someone truly cannot decide, caregivers must act in their best interests and choose the least restrictive option. That means protecting safety while respecting dignity, rights, wishes, and independence.
The Mental Capacity Act 2005 gives caregivers a practical rule for everyday care: support the person first, assess carefully, record clearly, and never remove choice without a lawful reason.
Need Support Understanding Mental Capacity in Care?
Making the right decision for someone who may lack capacity can feel difficult, especially when safety, dignity, family concerns, and legal responsibilities all matter at the same time.
At Care Sync Experts, we help caregivers, families, and care providers understand important care topics in clear, practical language. Our goal is to make complex guidance easier to apply in real care situations, from supporting daily choices to recognising when a best-interest decision may be needed.
If you care for someone who struggles with decisions about personal care, medication, safety, home routines, or moving into a care setting, do not guess your way through it. Learn the principles, ask the right questions, record clearly, and seek professional guidance when risks increase.
Care Sync Experts provides care-focused insights, practical care guidance, and evidence-based resources to support safer, more confident care decisions every day.
FAQ
What are the 5 principles of care?
The five commonly used principles of care are dignity, independence, privacy, choice, and safety. In practice, this means carers should treat people with respect, support them to do what they can for themselves, protect their personal information and private space, involve them in decisions, and reduce avoidable risks.
Skills for Care also highlights values such as individuality, independence, privacy, partnership, choice, dignity, respect, and rights as part of person-centred care.
What are the 5 C’s in care?
People often ask about the 5 C’s in care, but in UK health and social care the more recognised framework is the 6 C’s: care, compassion, competence, communication, courage, and commitment. NHS England introduced these values to describe the behaviours expected from nursing, midwifery, and care staff.
What are the 7 principles of care?
The seven principles of care usually refer to values such as dignity, independence, privacy, choice, safety, equality, and inclusion. These principles help care workers provide support that respects the person, protects their rights, and keeps them involved in decisions about their care.
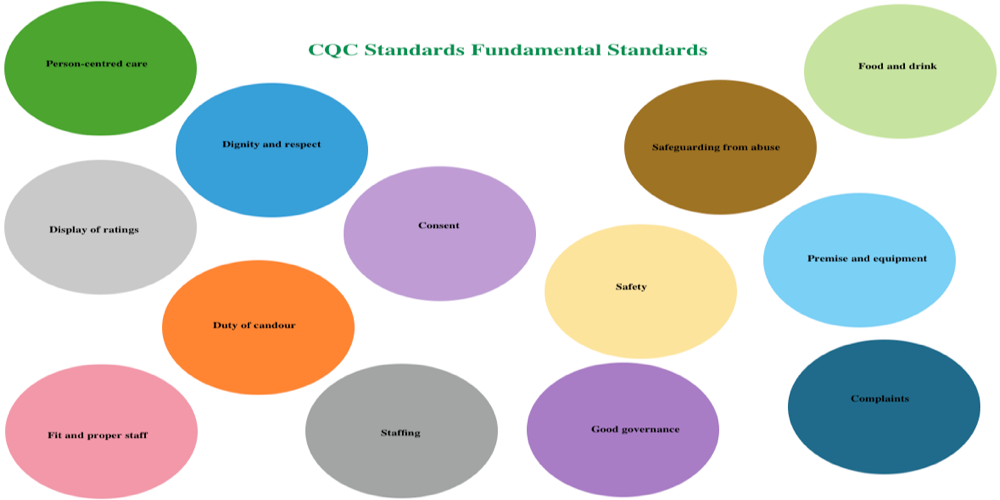
CQC guidance also stresses that providers must treat people with dignity and respect while they receive care and treatment.
What is Section 5 of the Mental Capacity Act?
Section 5 of the Mental Capacity Act 2005 covers acts done in connection with a person’s care or treatment when that person lacks capacity to consent. In simple terms, it can protect carers and professionals from liability when they reasonably believe the person lacks capacity and they act in the person’s best interests.
It does not allow careless or unnecessary restrictions; workers must still follow the MCA principles and choose the least restrictive option.