Yes, a bladder infection can cause nausea, but it usually happens when the infection becomes more severe or spreads beyond the bladder. A simple lower urinary tract infection (UTI) typically causes urinary symptoms, but nausea often signals that the infection may have reached the kidneys or triggered a stronger body response.
This article will answer the popular question care workers mostly ask: will a bladder infection cause nausea. Caregivers should pay close attention when nausea appears alongside a UTI, as this may indicate a more serious condition that requires prompt medical treatment.
A urinary tract infection does not usually affect the stomach directly. However, certain changes in the body can trigger nausea, especially when the infection becomes more severe.
Infection Spreads to the Kidneys
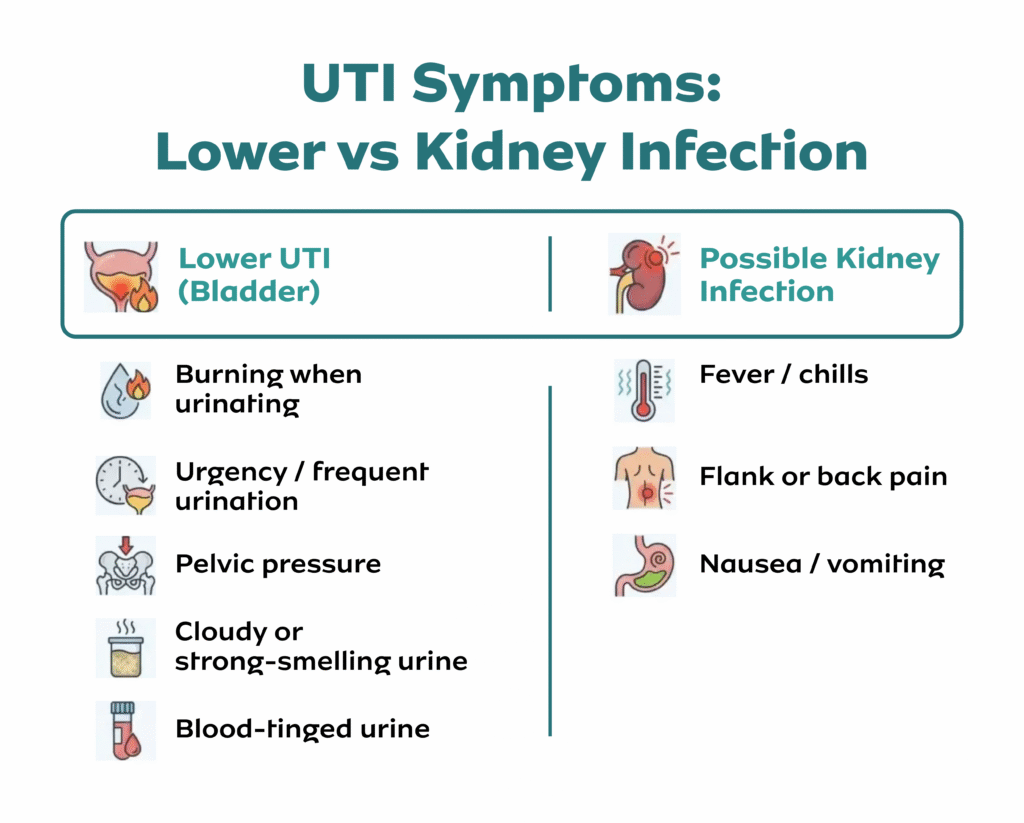
When bacteria move from the bladder to the kidneys, the infection becomes more serious (pyelonephritis). This stage often causes nausea, vomiting, fever, and back pain. Caregivers should treat this as urgent.
Strong Immune Response
The body reacts to infection by releasing inflammatory chemicals. This response can make a person feel unwell, tired, and nauseous. In some cases, the discomfort feels similar to flu symptoms.
Medication Side Effects
Some UTI antibiotics, such as nitrofurantoin, can cause nausea as a side effect. This does not always mean the infection is worsening, but caregivers should monitor symptoms closely.
Underlying Bladder Infection Causes
Different bladder infection causes, such as bacterial overgrowth, poor hygiene, or incomplete bladder emptying, can influence how severe the infection becomes. In women, understanding what causes a UTI in a woman (like shorter urethra or hormonal changes) helps explain why symptoms can escalate quickly.
For caregivers, the key takeaway is simple: nausea is not usually the first sign of a UTI, but when it appears, it often signals that the infection needs closer attention or medical review.
When Nausea Means Something Serious
Nausea alone does not always signal danger, but when it appears with certain symptoms, caregivers should act quickly. These combinations often point to a more serious infection, especially one affecting the kidneys.
Red Flags to Watch For
Fever and chills
Lower back or side pain
Vomiting or inability to keep fluids down
Severe fatigue or confusion (common in older adults)
Painful or frequent urination alongside worsening symptoms
These signs suggest the infection may have progressed beyond a simple bladder infection and now requires urgent treatment urinary tract infection care.
Special Situations Caregivers Must Not Ignore
UTI in pregnancy: Even mild symptoms can become serious quickly and require immediate medical attention.
Recurrent infections: If someone experiences repeated UTIs, caregivers may wonder, can recurrent UTIs be a sign of cancer? While this is rare, persistent infections should always be medically evaluated to rule out underlying conditions.
Caregiver Insight
Do not wait for symptoms to “settle.” If nausea appears alongside any of these warning signs, seek medical care immediately. Early intervention with proper urine infection treatment can prevent complications and speed up recovery.
A urinary tract infection often starts with mild, easy-to-miss symptoms. Caregivers should spot these early to prevent the infection from worsening.
General UTI Symptoms
Frequent urge to urinate
Burning sensation when urinating
Cloudy or strong-smelling urine
Lower abdominal or pelvic pain
Fatigue or general discomfort
These symptoms usually point to a lower UTI (bladder infection). When symptoms escalate, the risk of complications increases.
UTI Symptoms in Women
Women experience UTIs more often due to anatomy and hormonal factors. Many caregivers ask about the 10 causes of UTI in females, which commonly include poor hygiene, dehydration, sexual activity, and incomplete bladder emptying.
Understanding what causes a UTI in a woman helps caregivers act early and prevent recurrence. Women may also report pelvic pressure and a constant urge to urinate, even after emptying the bladder.
UTI Symptoms in Men
Although less common, UTI in men can be more serious and often linked to underlying conditions.
Caregivers should watch for:
Painful urination
Lower abdominal or rectal discomfort
Weak urine flow
Fever in more advanced cases
Questions like can guys get urinary tract infections, do males get UTIs, or does man get UTI come up often, the answer is yes, and when they do occur, they require careful attention.
Understanding male UTI symptoms and how a man gets a urinary tract infection (such as through prostate issues or urinary blockages) helps caregivers respond appropriately and seek timely care.
How to Treat a UTI (Caregiver Action Plan)
Why UTI Can Persist After Antibiotics
Caregivers play a key role in getting fast, effective treatment. Early action prevents complications and speeds up recovery.
Medical Treatment (First-Line Care)
Doctors treat most UTIs with antibiotics. Start treatment as soon as symptoms appear and follow the full course.
Common options include nitrofurantoin, trimethoprim, and cephalexin
Many people ask, what is best antibiotic for urinary tract infection, the best choice depends on the bacteria and the patient’s history
UTI antibiotics usually begin to relieve symptoms within 24–72 hours
If you’re wondering how long does nitrofurantoin take to work on a UTI, most patients feel improvement within 2–3 days
Caregivers should ensure the patient:
Takes medication exactly as prescribed
Finishes the full course, even if symptoms improve
Reports worsening symptoms immediately
This is the most reliable treatment urinary tract infection approach.
UTI Treatment at Home (Supportive Care)
Home care supports recovery but does not replace antibiotics for most infections.
Encourage plenty of fluids (water helps flush bacteria)
Promote regular urination (do not hold urine)
Maintain proper hygiene
Ensure adequate rest
Many caregivers search for UTI treatment at home or how to treat a UTI naturally. While these steps help, they do not cure most infections alone.
Common Questions Caregivers Ask
Can a UTI heal on its own?
Mild cases may improve, but most require antibiotics to prevent complications
How to get rid of a UTI in 24 hours?
There is no guaranteed way, fast treatment reduces symptoms, but full recovery takes a few days
How to get rid of cystitis fast?
Start antibiotics early, stay hydrated, and rest
Water infection tablets:
Over-the-counter products may relieve symptoms, but do not replace proper urine infection treatment
Caregivers should always prioritize early medical care. Quick action reduces the risk of the infection spreading and helps patients recover safely.
Some patients face a higher risk of complications from a urinary tract infection. Caregivers must act faster and monitor symptoms more closely in these situations.
Elderly Patients
Older adults may not show typical UTI symptoms. Instead, they may develop:
Confusion or sudden changes in behavior
Increased weakness or falls
Loss of appetite
Do not assume these signs are “normal aging.” A UTI can quickly worsen without obvious urinary symptoms.
UTI in Pregnancy
A UTI in pregnancy requires immediate attention. Even mild symptoms can lead to serious complications, including kidney infection or premature labor.
Caregivers should:
Encourage early testing
Ensure prompt treatment
Never delay medical care
Recurrent UTIs
Frequent infections should not be ignored. Many caregivers ask, can recurrent UTIs be a sign of cancer? While this is uncommon, repeated infections can signal underlying issues such as:
Kidney stones
Structural problems in the urinary tract
Chronic bladder conditions
A healthcare provider should always investigate persistent or recurring UTIs.
UTIs in Men
Although less common, male UTI cases often indicate an underlying condition such as prostate enlargement or urinary blockage.
Caregivers should pay attention to:
Persistent symptoms
Difficulty urinating
Recurrent infections
Understanding 10 causes of UTI male (such as poor bladder emptying, catheter use, or prostate issues) helps caregivers recognize when further evaluation is needed.
In all these cases, do not rely on home remedies alone. Early diagnosis, proper treatment urinary tract infection, and close monitoring can prevent serious complications.
Caregivers should not wait when symptoms worsen. A urinary tract infection can escalate quickly, especially when nausea is involved.
Seek urgent care if the person has:
Nausea with vomiting
Fever or chills
Lower back or side pain
Severe weakness or confusion
Inability to keep fluids or medication down
Symptoms that do not improve after starting UTI antibiotics
These signs often indicate a kidney infection or a more serious complication.
Delaying care can allow the infection to spread into the bloodstream (sepsis), which can become life-threatening. Early treatment urinary tract infection reduces this risk and improves recovery outcomes.
Caregiver Tip
If you are unsure, do not guess; get a UTI test done as soon as possible. Testing confirms the infection and helps doctors choose the right urine infection treatment quickly.
Final Thoughts…
So, will a bladder infection cause nausea? Yes, but it often signals that the infection has become more serious or is affecting the kidneys. Caregivers should never ignore this symptom, especially when it appears with fever, vomiting, or back pain.
The key to managing any UTI is early action. Start proper urine infection treatment quickly, monitor symptoms closely, and seek medical care when warning signs appear. While UTI treatment at home can support recovery, it should never replace medical care when symptoms worsen.
Stay alert, act early, and always prioritize safety. Quick decisions and proper care can prevent complications and help patients recover faster.
Need Help Managing UTIs in Your Care Service?
If you want to avoid delayed treatment, worsening symptoms, and preventable complications, expert guidance can make a real difference in how you manage infections like UTIs.
Care Sync Experts supports care providers and caregivers with:
practical guidance on recognising early UTI symptoms
support with infection prevention and care protocols
staff training on managing common conditions like UTIs
clear escalation pathways for high-risk cases
ongoing compliance support aligned with current care standards
We understand how quickly a simple infection can escalate, especially in vulnerable patients, and we help you stay prepared with the right systems and knowledge.
If you want to strengthen your care processes or improve how your team handles infections, speak to our team today.
This guide was prepared by Care Sync Experts and reflects best practices as of 2026. Always seek medical advice from a qualified healthcare professional for diagnosis and treatment.
FAQ
What can be mistaken for a bladder infection?
Several conditions can feel like a bladder infection, including vaginal infections (like yeast infections), sexually transmitted infections (STIs), kidney stones, or interstitial cystitis (a chronic bladder condition). Caregivers should not assume; it’s best to confirm with a proper UTI test to avoid treating the wrong condition.
What is the first stage of a UTI?
The first stage usually begins in the lower urinary tract (bladder or urethra). Early signs include a frequent urge to urinate, mild burning, and discomfort in the lower abdomen. Acting at this stage makes treatment urinary tract infection easier and prevents the infection from spreading.
What not to drink when having a UTI?
Avoid drinks that irritate the bladder, such as caffeine (coffee, tea), alcohol, and sugary or fizzy drinks. These can worsen symptoms and delay recovery. Caregivers should encourage water, which supports effective urine infection treatment.
Can you have a UTI without burning during urination?
Yes, not everyone experiences burning. Some people, especially older adults, may only show symptoms like fatigue, confusion, nausea, or general discomfort. Caregivers should stay alert, as UTIs can present differently depending on the individual.
The Care Quality Commission (CQC) has, since July 1st, 2025, changed how it handles new homecare applications, and the impact has been brutal for unprepared providers.
CQC now routinely returns and rejects incomplete or inaccurate domiciliary care applications at the point of receipt. When that happens, any resubmission counts as a brand-new application. You lose your place in the queue. You start again from the back. In some cases, that mistake adds months to your launch timeline.
This single procedural change in CQC registration for domiciliary care providers explains why so many new CQC domiciliary care applications are failing right now.
The rules did not get easier. CQC raised the bar, deliberately.
Most online guides still teach the old approach:
“Submit what you have and fix issues later.”
“CQC will come back with questions.”
“Minor errors won’t matter.”
That advice is now dangerous.
CQC no longer treats missing documents, outdated forms, or vague answers as fixable issues. They treat them as grounds for immediate rejection.
If your application fails at intake:
CQC does not correct it with you
CQC does not hold your place
CQC applies whatever new requirements exist at resubmission
That last point matters more than people realise. Requirements continue to evolve. A delay today can mean more documents, more scrutiny, and more cost tomorrow.
Why CQC Tightened the Process
Do You Really Need CQC Registration for Supported Living? | 2026 Guide for Providers
CQC did not make this change randomly.
An independent operational review (the Dash review) exposed severe backlogs and inefficiencies. More than half of new provider applications were missing basic information. Some sat unresolved for months. Instead of absorbing that burden, CQC redesigned the process to filter weak applications immediately.
The result is a strict two-stage system:
Initial checks that act as a hard gate
Full assessment only for applications that pass cleanly
We’ll break both stages down in detail later in this guide.
What This Guide Does Differently
This is not a generic overview of CQC registration for domiciliary care providers.
This guide focuses on:
How CQC actually assesses applications today
Where applications fail before assessment even begins
The exact submission mechanics that cause avoidable rejection
The documents, detail, and consistency CQC now expects from day one
If you plan to apply for CQC registration in 2026, read this guide carefully and follow it in order.
Who Needs to Register With CQC for Domiciliary Care?
If you plan to deliver personal care in people’s own homes, the law leaves no room for interpretation. You must register with the Care Quality Commission before you provide any care.
CQC does not assess intentions. They assess what you actually do.
What Counts as Domiciliary Care?
Domiciliary care (also called homecare) involves supporting people in their own homes with tasks they cannot safely do alone. This includes:
Helping with washing or bathing
Assisting with dressing
Supporting eating and drinking
Helping people take medication
Providing personal hygiene support
If your service includes any of these activities, CQC classifies it as personal care, which is a regulated activity under the Health and Social Care Act 2008.
Who Is Legally Required to Register?
You must register if you provide personal care as:
A limited company
A partnership
A sole trader/individual
A charity or non-profit organisation
CQC does not care about your business size. A one-person homecare startup must meet the same registration standard as a multi-branch provider.
Who Does Not Need to Register?
Some providers assume they need registration when they don’t, while others assume the opposite and get it wrong.
You do not need to register with CQC if you only provide:
Domestic help (cleaning, shopping, laundry)
Companionship or social support without personal care
Administrative or care coordination services only
The moment you cross into hands-on personal care, registration becomes mandatory.
What About Managers and Individuals?
CQC registration applies at two levels:
The provider organisation or individual
The registered manager (a separate regulated role)
If you operate alone, you may act as:
the provider
the nominated individual
the registered manager
CQC allows this, but it increases scrutiny. You must clearly explain how you manage governance, accountability, and complaints when one person holds multiple roles. We’ll cover this in detail later.
Operating Without Registration Is an Offence
Providing regulated care without registration is not a minor breach. It is a criminal offence.
CQC has enforcement powers that include:
prosecution
fines
enforcement notices
long-term impact on future registration attempts
If you plan to offer personal care, you should not market, recruit staff, or accept clients until CQC confirms your registration.
Quick Self-Check: Do You Need to Register?
You need CQC registration now if:
You will help people wash, dress, eat, or take medication
You advertise personal care services
You employ or plan to employ care workers for personal care
If any of these apply, registration is not optional.
Registering With CQC as an Individual (Sole Trader)
Registering with the Care Quality Commission as an individual is legal, common, and fully permitted. However, it is not the easier option, despite what many people assume.
CQC applies the same regulatory standards to individual providers as it does to limited companies. In practice, individual applicants often face closer questioning, not less.
What Stays the Same
If you register as an individual rather than a company, these requirements do not change:
Personal care remains a regulated activity
You must meet all fundamental standards
You must submit the same core supporting documents
You must demonstrate safe care, governance, and financial sustainability
CQC does not lower expectations because you are a sole trader.
What Changes for Individual Providers
Where things differ is how CQC evaluates responsibility and oversight.
When you register as an individual:
You become the legal provider
You carry personal accountability for compliance
CQC expects clear evidence of how you manage risk, quality, and decision-making
If you also act as the registered manager, CQC will examine how you separate:
operational delivery
governance oversight
complaints handling
You must show that one person can realistically manage all three without conflicts of interest.
The Governance Challenge (Where Many Applications Fail)
CQC often rejects individual applications because governance is poorly explained.
Common weak answers include:
“I will manage everything myself”
“I will deal with complaints if they arise”
“I will monitor quality regularly”
These statements say nothing about how you will do those things.
As an individual provider, CQC expects you to explain:
how you audit care quality
how you identify risks
how you act on feedback
how complaints about you are handled independently
If you cannot show this clearly in your governance and complaints policies, your application is unlikely to pass.
Individual vs Limited Company: Practical Differences
Choosing to register as an individual affects more than paperwork.
Individual registration means:
You carry personal liability
You rely heavily on your own experience and competence
You must demonstrate credibility without a wider management structure
Limited company registration allows:
clearer separation of governance and operations
easier delegation as the service grows
stronger perception of sustainability for CQC assessors
CQC does not tell you which route to choose, but it does assess whether your chosen structure makes sense for the service you propose.
When Individual Registration Makes Sense
Registering as an individual may be appropriate if:
You have strong prior care management experience
You plan to run a small, local service initially
You fully understand the compliance burden
You can clearly explain governance arrangements
If you lack experience or plan rapid growth, individual registration often creates avoidable risk.
How CQC Processes New Domiciliary Care Applications in 2026
The biggest mistake new providers make is assuming CQC registration works the way it did a few years ago.
It doesn’t.
On 1 July 2025, the Care Quality Commission fundamentally changed how it processes new domiciliary care applications. That change still governs approvals in 2026.
The Old Assumption (Now Wrong)
Before mid-2025, many applicants believed:
CQC would flag missing documents later
Minor errors could be corrected during assessment
Applications stayed in the queue while issues were fixed
That approach no longer applies.
The New Reality
CQC now applies strict intake controls.
When your application arrives, CQC first checks whether:
every required document is present
all forms are current and fully completed
the information is accurate and internally consistent
If anything fails at this point, CQC returns or rejects the application immediately.
There is no partial acceptance. There is no “we’ll fix this later.”
Why Resubmission Is So Risky
If CQC rejects your application at intake:
you must correct the issues
you must resubmit everything
CQC treats the resubmission as a new application
That means:
you lose your original place in the queue
your timelines reset
any new requirements introduced meanwhile apply to you
In practical terms, one missing document can delay your launch by months.
Why CQC Made the Process Stricter
CQC tightened the system after an operational review revealed widespread problems:
high volumes of incomplete applications
long processing delays
assessors spending time chasing basic information
Instead of absorbing that inefficiency, CQC redesigned the process to filter out weak or unprepared applications immediately.
This protects their resources, and shifts the burden onto providers to submit complete, assessment-ready packs from day one.
What This Means for You
CQC no longer rewards “good enough” submissions.
To succeed in 2026, your CQC domiciliary care application must:
arrive complete
follow current guidance exactly
include documents that meet minimum requirements
show consistency across every form and policy
If your pack does not meet those standards at intake, CQC will not progress it.
That is why preparation now matters more than speed.
The Two-Stage CQC Domiciliary Care Application Process
Every CQC domiciliary care application now passes through two distinct stages. Each stage has a different purpose, and a different failure risk.
Understanding the difference is essential if you want to register successfully.
1. Stage One: Initial Checks (Where Most Applications Fail)
Stage One is not an assessment of care quality. It is a gatekeeping exercise.
When the Care Quality Commission receives your application, they first check whether it is complete, current, and assessable.
At this stage, CQC looks for one thing only: Can this application move forward without further clarification?
What CQC Checks at Stage One
CQC will confirm that:
All required application forms are included
Every form uses the latest version
All sections of every form are fully completed
All required supporting documents are attached
Documents meet minimum content requirements
Information is consistent across forms and policies
This is a strict yes-or-no decision.
If even one required document is missing, or one form uses an outdated version, CQC will reject the application.
What Stage One Is Not
CQC does not:
review care quality in depth
interview your manager
assess how well your policies work in practice
That comes later.
Stage One exists to filter out incomplete or poorly prepared submissions.
Why Applications Fail at Stage One
Most rejections at this stage happen because of:
Missing supporting documents
Incorrect or outdated forms
Blank fields or vague answers
Generic policies that lack required detail
Contradictions between documents
Email submission errors
CQC will usually email you to explain why your application was rejected, but by then the damage is done.
If you resubmit, CQC treats it as a new application.
Stage One Pass Checklist (Use This Before You Submit)
Your application should pass Stage One if:
Every required document is included
Every form is current and fully completed
No answers are left blank
Policies reflect your actual service model
Your Statement of Purpose, business plan, and policies align
File names are clear and organised
All documents are submitted together
If you cannot confidently tick all of these, do not submit yet.
2. Stage Two: Full Assessment (Where CQC Tests Your Readiness)
Only applications that pass Stage One move to Stage Two.
Stage Two is where CQC evaluates whether you are fit to provide safe, effective, and well-led care.
This is a detailed assessment, not a tick-box exercise.
What CQC Assesses at Stage Two
During full assessment, CQC will review:
Your supporting documents in detail
Your understanding of the fundamental standards
Your governance and quality assurance systems
Your safeguarding arrangements
Your recruitment and training processes
Your financial sustainability
Your ability to manage risk and respond to incidents
CQC may also:
request additional information
conduct a registration interview
arrange a premises visit to your office base
The Registration Interview
CQC often interviews the registered manager and sometimes the nominated individual.
They expect you to:
explain how your policies work in practice
demonstrate understanding of safeguarding and medicines management
show how you monitor quality and learn from issues
answer confidently without contradicting your documents
CQC does not expect perfection, but they do expect competence and honesty.
Premises Visits for Homecare Providers
Even though care takes place in people’s homes, CQC may visit your registered office base.
They will check:
health and safety arrangements
secure storage of records
readiness to operate
evidence of legal occupancy
If your premises are not ready when visited, CQC may refuse your application.
Why Stage Two Takes Time
Stage Two can take several months. CQC assesses risk carefully and may handle many applications at once.
You must:
respond quickly to information requests
monitor your email daily
keep your documents consistent
CQC may give you only a few days to respond to requests. Delays or incomplete responses can stall or damage your application.
In Short…
Stage One decides whether CQC will even assess you. Stage Two decides whether you are fit to provide care.
Most providers focus too much on Stage Two and underestimate Stage One. In 2026, Stage One is where most applications fail.
Documents Required for CQC Registration (2026 Homecare Pack)
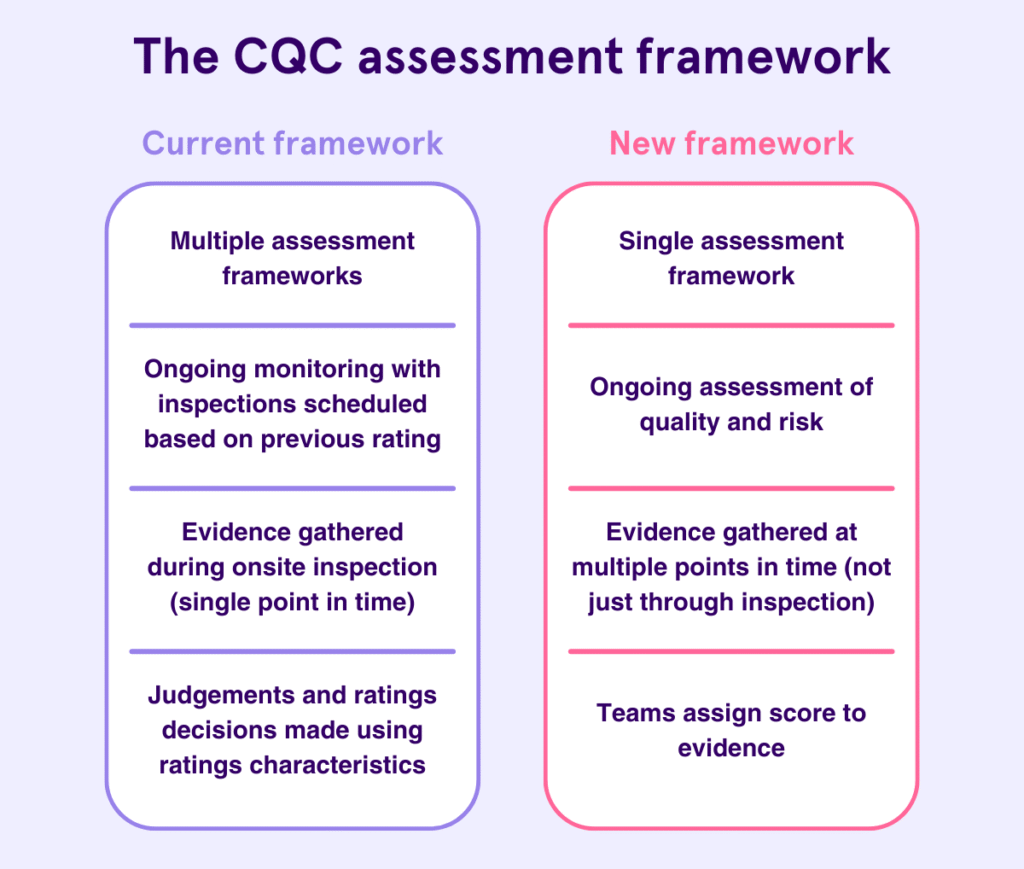
CQC Assessment Framework
CQC does not reject domiciliary care applications because providers lack good intentions. They reject them because documents are missing, weak, inconsistent, or unassessable.
If your document pack does not meet minimum requirements, the Care Quality Commission will return your application before assessment begins.
This section explains exactly what you must submit, and what CQC expects to see inside each document.
Core Documents Required for All Providers
Every provider applying for CQC registration must submit the following. There are no exceptions.
Statement of Purpose
Your Statement of Purpose defines your service. CQC cross-checks it against every other document.
It must clearly explain:
the regulated activities you will provide
who you will support
where services will be delivered
how care will be delivered
CQC expects this document to be:
service-specific
current
consistent with your business plan and policies
If your Statement of Purpose describes services your policies do not support, your application will fail.
DBS Checks
You must provide enhanced DBS checks for:
the provider (if an individual)
the nominated individual
the registered manager
DBS certificates must:
be countersigned where required
be less than 12 months old at submission
Start DBS applications early. Delays here stall entire applications.
Insurance Evidence
You must submit evidence of:
public liability insurance
employer liability insurance (if you will employ staff)
CQC only accepts one insurance document. If you require both types, you must complete the CQC liability insurance supporting information form and include your certificates.
Expired or incorrect insurance evidence leads to rejection.
Additional Documents Required for Domiciliary Care Providers
If you are registering to provide personal care, CQC requires additional service-specific documents.
These are non-negotiable.
Additional Information for Providers of Personal Care (Form)
This form is mandatory for homecare providers.
CQC uses it to assess:
how you recruited key personnel
how you assessed competence
whether genuine local demand exists for your service
Weak answers here often expose:
lack of market research
unrealistic service plans
governance gaps
Treat this form as an assessment tool, not an admin exercise.
Business Plan (With Financial Forecast)
Your business plan must demonstrate that your service is viable and sustainable.
CQC expects:
clear service model explanation
evidence of local market demand
realistic staffing plans
a one-year financial forecast
a SWOT analysis
Vague statements like “there is demand for care services” will not pass. CQC expects evidence, not assumptions.
Evidence of Legal Occupancy
You must prove you have permission to operate from your registered address.
Acceptable evidence includes:
title deeds (if you own the property)
tenancy or licence agreement
written permission from landlord or mortgage provider
This applies even if you operate from home. Missing or unclear occupancy evidence is now a common rejection reason.
Staff Training Plan
CQC no longer accepts a simple training matrix.
Your training plan must explain:
induction training
mandatory training
refresher schedules
specialist training where required
support for overseas workers
who delivers the training
CQC wants to see how training works in practice, not just a list of topics.
Service User Guide
This document explains your service to people who use it.
It must cover:
what services you offer
pricing and charges
safeguarding information
how to raise concerns or complaints
If this document reads like marketing copy instead of practical guidance, CQC will challenge it.
Policies Required for All Home Care Providers
CQC requires a specific policy set. Each policy must reflect how your service actually operates.
You must submit policies covering:
consent
equality, diversity and human rights
governance
infection prevention and control
medicines management
recruitment
safeguarding
complaints
Generic templates often fail because they:
describe services you do not provide
contradict your Statement of Purpose
lack sufficient operational detail
CQC cross-checks policies line by line. Inconsistencies trigger rejection.
Minimum Requirements: What CQC Means by “Assessable”
CQC’s guidance is clear. Documents must include enough detail to be assessed.
That means:
no placeholders
no blank sections
no copied text that does not apply to your service
no contradictions between documents
If an assessor cannot understand how your service will operate, your application does not progress.
Final Document Pack Self-Check
Before submission, confirm that:
every required document is included
every document reflects your service model
all documents agree with each other
all documents use current terminology
nothing relies on “we will decide later”
If any document fails this test, fix it before you submit.
CQC Application Form for New Providers: What to Prepare Before You Fill It In
Many domiciliary care applications fail before CQC reads a single policy.
The problem is not the documents. The problem is the CQC application form for new providers.
The Care Quality Commission uses this form as the master reference point. Assessors cross-check everything else against it. If the form contains vague answers, missing detail, or contradictions, CQC rejects the application at Stage One.
Do Not Start the Form Until These Decisions Are Final
Before you touch the application form, you must lock down the following:
Regulated activity For homecare agencies, this is usually personal care. Do not list activities you are not ready to deliver.
Service model Who you will support, how you will deliver care, and what you will not provide.
Registered location Your office base address must be final and supported by legal occupancy evidence.
Key roles Who is the provider, nominated individual, and registered manager, and whether any roles overlap.
If any of these points remain undecided, stop. Incomplete thinking here leads to rejection later.
How CQC Reads Your Application Form
CQC does not read the form in isolation.
Assessors compare it against:
your Statement of Purpose
your business plan
your policies and procedures
the additional personal care form
If your form says one thing and your documents say another, CQC assumes you do not understand your own service.
That is a red flag.
Common Form Errors That Trigger Rejection
CQC regularly rejects applications because the form includes:
Blank fields Every question must be answered. If something does not apply, state “Not applicable” and explain why.
Vague language Phrases like “we will ensure”, “we plan to”, or “we intend to” without explanation show lack of readiness.
Overly broad services Listing services you cannot evidence through policies, training, or staffing.
Inconsistent answers For example, describing a small, local service in one section and a large multi-area operation in another.
Outdated assumptions Using terminology or processes that no longer reflect current CQC expectations.
Each of these issues can stop your application before assessment begins.
How to Write Strong Answers (What CQC Expects)
Strong answers are:
specific
consistent
evidence-backed
Instead of writing:
“We will provide high-quality care tailored to individual needs.”
Write:
“We will deliver personal care to adults in their own homes within [location], following care plans developed after initial assessment and reviewed monthly.”
Clarity beats ambition every time.
The “Cross-Check Rule” (Use This Before Submission)
Before you submit the application form, cross-check each answer against:
your Statement of Purpose
your business plan
your policies
If any answer cannot be supported by a document, revise it.
CQC assumes:
If it is written in the form, you must already be able to deliver it.
Final Form Readiness Checklist
Your application form is ready when:
every field is completed
no answers rely on future decisions
language matches your documents exactly
service scope is clear and realistic
roles and responsibilities are consistent
If you rush this stage, CQC will return your application, and you will lose your place in the queue.
How to Apply for CQC Registration (Submission Mechanics That Make or Break You)
What is CQC Registration?
Many providers prepare strong documents and still fail because they submit their CQC domiciliary care application incorrectly.
At this stage, CQC does not troubleshoot. If your submission does not meet their technical requirements, your application may never reach assessment.
You must email your complete application bundle to:
HSCA_Applications@cqc.org.uk
CQC requires email submission for new provider applications. This is not optional.
The 10MB Email Size Rule (Non-Negotiable)
CQC can only receive emails up to 10MB in size.
This includes:
all attachments
the email body
embedded signatures
If your email exceeds 10MB:
CQC may not receive it at all
you may not get a bounce-back warning
your application may be treated as missing
If your application exceeds 10MB, you must split it into multiple emails.
Correct Subject Line Format (Critical for Multi-Email Submissions)
When sending more than one email, CQC requires a specific subject line format so they can match your documents correctly.
Use this format exactly:
[Provider Name] new provider application 1/2 [Provider Name] new provider application 2/2
If you send three emails, use 1/3, 2/3, 3/3.
If you do not follow this format:
emails may not be linked together
CQC may treat your application as incomplete
your application may be rejected at intake
This is one of the most common and avoidable failures.
All Documents Must Arrive Together
CQC requires that all documents arrive at the same time.
You cannot:
send the application form today
send policies tomorrow
send missing documents next week
If anything is missing from the initial submission, CQC will return or reject the application.
When you resubmit, it counts as a new application.
File Naming and Organisation (Make Review Easy)
CQC assessors review large volumes of applications. Clear organisation helps your application move smoothly.
Use:
separate files for each document
clear, descriptive file names
consistent terminology across documents
Good example:
Statement of Purpose – Oxtown Care Ltd.pdf
Safeguarding Policy – Domiciliary Care.pdf
Business Plan – Homecare Services.pdf
Avoid:
vague names like “Policy 1”
merged documents containing multiple policies
zipped folders unless absolutely necessary
Assessors must be able to locate documents quickly.
What to Include in the Email Body
Keep the email body simple and factual.
Include:
provider name
confirmation that this is a new provider application
number of emails being sent (if applicable)
Do not include explanations, justifications, or attachments that are not required.
Submission Day Checklist (Use This Before You Click Send)
Before submitting, confirm that:
All required documents are attached
All forms use the latest versions
File names are clear and consistent
Total email size is under 10MB
Subject line format is correct
All emails are ready to send together
If any item is missing, stop and fix it first.
After You Submit: What to Do Next
After submission:
save sent emails and attachments
keep a copy of everything submitted
monitor your inbox daily
CQC may contact you quickly if there is an issue. Delayed responses can slow your application or affect assessment.
Note: Strong documents mean nothing if CQC cannot process your submission.
Follow the submission mechanics precisely. Treat this step with the same seriousness as the documents themselves.
Why CQC Rejects Domiciliary Care Applications (And How You Prevent It)
Most failed applications do not fail because providers lack experience or commitment. They fail because applicants underestimate how precise and unforgiving the Care Quality Commission has become.
Below are the rejection reasons we see most often, and exactly how to avoid each one.
Rejection Reason 1: Missing Documents
This is the single biggest cause of rejection. If even one required document is missing, CQC will return or reject your application at intake.
How to prevent it
Use a master document checklist before submission
Confirm every required document is attached
Do not assume CQC will “ask for it later”
CQC will not chase missing documents anymore.
Rejection Reason 2: Using Outdated Forms
CQC updates application forms periodically. Submitting an old version triggers immediate rejection.
This includes:
provider application forms
manager application forms
additional personal care forms
How to prevent it
Download every form directly from the CQC website immediately before completing it
Never reuse forms from old applications or third-party packs
If the form version is wrong, nothing else matters.
Rejection Reason 3: Incomplete or Vague Form Answers
Leaving fields blank or providing vague responses signals unreadiness.
CQC does not accept:
empty fields
“to be confirmed” answers
generic statements without explanation
How to prevent it
Answer every field
If something does not apply, state “Not applicable” and explain why
Replace vague language with specific operational detail
CQC interviews assess judgement, not just knowledge.
Interview Readiness Checklist
You are ready if you can:
explain your service model clearly
describe safeguarding processes confidently
walk through recruitment and training steps
explain how you monitor quality
discuss complaints handling realistically
If you cannot explain it verbally, CQC will question whether you can deliver it in practice.
After You Get Registered: What Happens Next (and How to Stay Inspection-Ready)
Once the Care Quality Commission grants registration, you can legally begin providing domiciliary care. But approval does not come with a grace period.
From day one, CQC expects you to operate exactly as described in your application.
What Changes Immediately After Registration
As soon as registration is confirmed:
You can start delivering regulated personal care
You become liable for annual CQC fees
You must comply fully with the regulations
Your service becomes eligible for inspection
CQC assumes that everything you described on paper is already in place and working.
Your First Inspection: What to Expect
CQC usually inspects new domiciliary care providers within the first 12 months of registration. However, inspections can happen sooner if CQC identifies risk.
Inspections focus on the five key questions:
Is the service safe?
Is it effective?
Is it caring?
Is it responsive?
Is it well-led?
Inspectors will test whether your service matches your registration documents in practice.
The First 30 Days: What You Should Do Immediately
The first month after registration sets the tone for inspection readiness.
You should:
implement all policies and procedures in real operations
begin staff supervision and competency checks
keep training records up to date
document care planning and reviews
log incidents, complaints, and actions taken
Do not wait for inspection to start recording evidence. Inspectors expect to see a working paper trail.
Maintain Compliance, Not Just Documents
Many providers pass registration and fail inspection because policies exist only on paper.
CQC expects to see:
staff following procedures
audits being completed
feedback being collected and acted upon
risks identified and managed
If your service looks different from what you described in your application, inspectors will challenge it.
Notify CQC of Changes
You must notify CQC about certain changes, including:
changes to your nominated individual or registered manager
changes to your registered address or premises
significant incidents or safeguarding concerns
changes to the services you provide
Failing to notify CQC is itself a compliance breach.
Keep Your Statement of Purpose Accurate
Your Statement of Purpose must stay current.
If your services change, you must:
update the document
ensure policies still align
notify CQC where required
Outdated Statements of Purpose are a common inspection finding.
Note: Registration confirms that you can provide care. Inspection confirms whether you do provide it safely and consistently.
Treat compliance as an ongoing process, not a one-off hurdle.
The CQC Registered Providers List: Why It Matters and What to Check
Once CQC approves your application, your service appears on the CQC registered providers list. This is not a formality. It is your public regulatory record.
Commissioners, local authorities, families, insurers, and partners use this register to verify whether a provider is legally allowed to operate.
What the CQC Register Shows
Your public listing typically includes:
your provider name
your registered address
your regulated activities
your registered manager (where applicable)
your inspection status and rating (once inspected)
This information becomes part of your public reputation.
Why the Register Matters for New Providers
For a new domiciliary care agency, the register:
proves you are legally registered
builds trust with service users and referrers
allows commissioners to verify compliance
confirms you can deliver regulated personal care
Many organisations will not engage with you until your registration appears on the public register.
What You Should Check as Soon as You Go Live
When your registration goes live, check your listing carefully.
Confirm that:
your provider name is correct
your address matches your legal occupancy evidence
your regulated activity is listed accurately
your service description reflects what you applied for
Errors happen. Leaving them uncorrected can cause confusion or delay referrals.
What to Do If Something Is Wrong
If you spot an error:
contact CQC promptly
provide clear evidence of the correction needed
keep records of communications
Do not assume CQC will fix mistakes automatically.
How the Register Connects to Inspection
Once registered, your listing links directly to:
inspection reports
ratings
enforcement history (if any)
Everything CQC publishes builds on your registration record. Accuracy matters from the start.
Check it. Maintain it. Treat it as part of your professional credibility.
Get Your CQC Registration Right the First Time
CQC registration for domiciliary care providers has changed, permanently.
Since July 2025, incomplete or inaccurate applications no longer move forward. CQC rejects them at the point of receipt. Resubmissions lose their place in the queue. Small mistakes now cost months, not days.
If you take one thing from this guide, take this: CQC no longer fixes applications. They filter them.
Success in 2026 depends on preparation, accuracy, and consistency, not speed.
You must:
submit the correct documents
use current forms
align every answer across your application
follow submission mechanics precisely
demonstrate readiness from day one
If any part of your application feels rushed, vague, or incomplete, stop and fix it before you submit.
Need Expert Help With Your CQC Registration?
If you want to avoid rejection, delays, and costly resubmissions, expert guidance can make the difference.
Care Sync Experts supports home care providers across England with:
Statement of Purpose and business plan development
application review before submission
registration interview preparation and coaching
ongoing compliance support after approval
We stay up to date with CQC regulatory changes, submission requirements, and assessment expectations, so you don’t have to learn the hard way.
Book a Free CQC Registration Consultation
If you’re planning to apply, or you’ve already faced rejection, speak to our team before you submit again.
This guide was prepared by Care Sync Experts and reflects current CQC requirements as of 2026. CQC guidance can change. Always verify current requirements with CQC before submitting your application.
FAQ
Is CQC Registration Difficult?
Most applications fail because providers: CQC registration is not difficult because it is complicated. It is difficult because it is precise. submit incomplete document packs contradict themselves across forms and documents misunderstand what “ready to operate” actually means.
The Care Quality Commission does not assess effort or intention. It assesses readiness and accuracy. If your application is complete, consistent, and specific to your service, registration is achievable. If it is vague or rushed, rejection is likely.
What Are the Different Types of CQC Registration?
CQC registration depends on what regulated activity you provide and how you operate, not on business size. For domiciliary care, the most common registrations are: Registered manager registration – required for the person managing day-to-day care delivery Provider registration – required for the organisation or individual delivering the service You may also register for different regulated activities, such as: personal care treatment of disease, disorder, or injury nursing care Each regulated activity carries different expectations and evidence requirements. You must only apply for activities you are genuinely ready to deliver
Do Private Carers Need to Be CQC Registered?
It depends on how the care is arranged. A self-employed carer does not need CQC registration if: they are directly employed by the person receiving care, and they do not operate through an agency or employ other carers However, registration is required if: care is arranged through an agency the carer employs staff the service provides regulated personal care as a business Many people get this wrong. Operating as an “independent carer” does not automatically remove the requirement to register
How Often Does CQC Inspect Domiciliary Care Providers?
CQC does not inspect on a fixed annual schedule. For new domiciliary care providers: the first inspection usually happens within 12 months of registration inspections can happen sooner if CQC identifies risk After that, inspection frequency depends on: previous inspection outcomes risk indicators intelligence or concerns raised CQC can also carry out unannounced inspections at any time. Providers must remain inspection-ready from the day they begin operating.
The SR1 form is a UK medical report used to support fast-tracked benefit claims for people with a terminal illness. A doctor or specialist completes the form to confirm that a patient has a progressive condition and may not live beyond 12 months.
The SR1 form replaced the DS1500 form, allowing eligible individuals to access higher-rate benefits more quickly without a medical assessment.
The SR1 form UK is used to fast-track benefit claims under special rules for terminal illness
It replaces the older DS1500 form (also known as DS1500)
A healthcare professional must complete the form; patients cannot fill it themselves
Claims supported by an SR1 form are processed faster and often qualify for higher payments
No face-to-face medical assessment is required in most cases
For care providers, understanding what is an SR1 form is essential. It helps you guide families through urgent financial support options and ensures clients receive the care they need without delays.
Care providers play a critical role in identifying when a client may need an SR1 form. Acting early can significantly improve a client’s access to financial support and ensure continuity of care during a difficult time.
When a client qualifies under the special rules, the sr1 form allows them to receive benefits quickly—often at the highest rate. This means families can afford consistent care services, whether that involves domiciliary care, specialist support, or additional staffing needs.
How the SR1 Form Supports Better Care Outcomes
Faster funding decisions: Clients receive financial support within days instead of weeks
Improved care planning: Providers can deliver services without delays caused by financial uncertainty
Reduced stress for families: Families focus on care and emotional support instead of complex benefit processes
Higher likelihood of sustained care packages: Access to enhanced benefit rates helps maintain long-term care arrangements
Your Role as a Care Provider
Care providers often notice changes in a client’s condition before anyone else. You can:
Recognise when a condition becomes life-limiting
Encourage families to speak with a GP or specialist
Ensure the sr1 process starts early to avoid delays in support
The earlier a care provider flags the need for an SR1 form, the faster a client can access the financial support required to maintain quality care.
By understanding what is an SR1 form and when to use it, care providers position themselves as trusted partners in both care delivery and client advocacy.
An SR1 form is a medical report completed by a healthcare professional to confirm that a patient has a progressive, life-limiting condition. It allows the Department for Work and Pensions (DWP) to process benefit claims under the special rules for terminal illness, without requiring a full medical assessment.
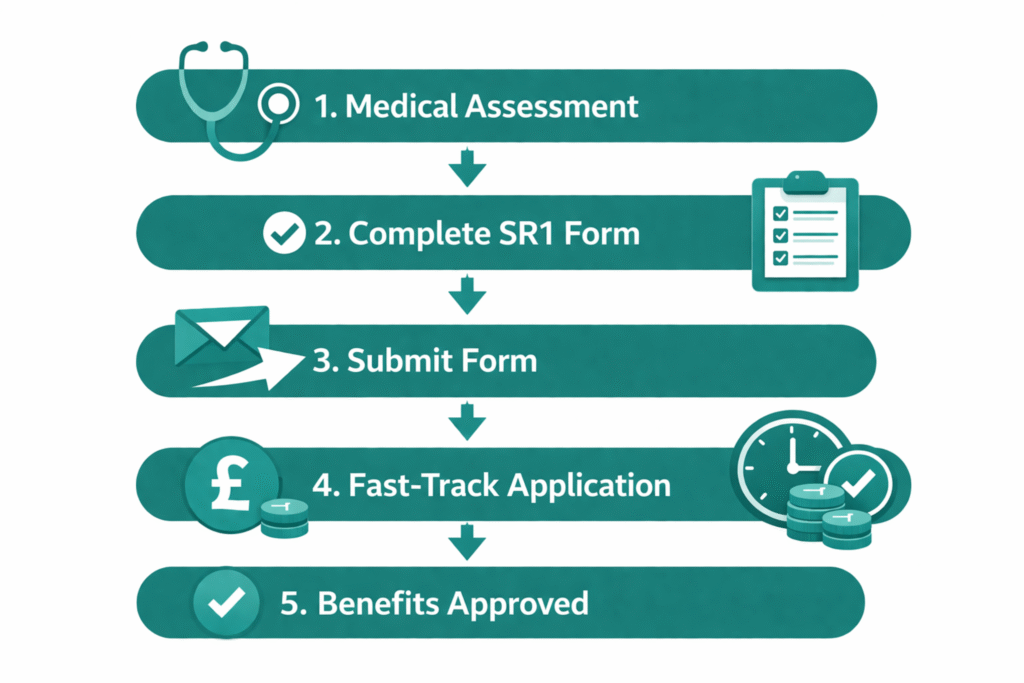
How the SR1 Process Works (Step-by-Step)
A clinician identifies eligibility
A GP, consultant, or specialist nurse determines that the patient has a progressive condition and may not live beyond 12 months.
The healthcare professional completes the SR1 form
The clinician records key medical details, including diagnosis, progression, and clinical indicators.
The SR1 form is submitted to the DWP
The form is usually sent directly by the clinician via secure systems or email.
The patient applies for benefits under special rules
The claim must clearly state that it is being made under the special rules for terminal illness.
The claim is fast-tracked and prioritised
Applications supported by an SR1 are processed quickly and often awarded at the highest rate.
Key Things to Know About How It Works
The sr1 form uk does not require a detailed life expectancy—clinicians use their professional judgment
The process focuses on speed, reducing delays in accessing support
The patient does not need to attend a medical assessment in most cases
The sr1 form acts as trusted medical evidence, allowing benefit decisions to be made quickly and with minimal stress for the patient and their family.
For care providers, understanding what is sr1 form and how it works helps you guide families through a time-sensitive process and ensures no unnecessary delays in securing essential support.
SR1 Form vs DS1500 Form: What Changed?
The SR1 form replaced the older DS1500 form to improve how people with terminal illnesses access benefits in the UK. While both forms serve the same purpose, supporting fast-tracked claims, the SR1 introduces a more modern, flexible, and clinician-friendly approach.
Key Differences Between SR1 and DS1500
Feature
SR1 Form
DS1500 Form
Status
Current system
Replaced (legacy)
Purpose
Fast-track benefit claims
Same purpose
Prognosis requirement
No strict timeline wording required
Previously more rigid
Submission
Digital, email, or post
Mostly paper-based
Clinician experience
Simplified and more flexible
More formal and restrictive
Improved access to support: The SR1 form makes it easier for clinicians to confirm eligibility without rigid wording
Faster processing: Digital submission options reduce delays compared to the ds1500 form
Better clinical judgment: Doctors can use professional discretion instead of fixed criteria
The transition from the DS1500 form to the SR1 form UK reflects a shift toward faster, more compassionate support for people with life-limiting conditions.
What Care Providers Should Know
Some families and even professionals may still refer to the ds1500, but it is no longer the standard
Always guide clients toward the sr1 form when applying under special rules
Understanding this change helps you avoid confusion and ensures the correct process is followed
By clearly explaining the difference between the SR1 form and the DS1500 form, care providers can support families more effectively and prevent delays in accessing critical benefits.
A patient qualifies for an SR1 form if they have a progressive, life-limiting condition, and a clinician would not be surprised if they were to live for less than 12 months. This definition focuses on clinical judgment rather than a strict prognosis, making the SR1 form UK more flexible and easier to apply in practice.
Core Eligibility Criteria
To qualify for an sr1 form, the patient must:
Have a progressive disease (the condition is worsening over time)
Be considered life-limiting by a healthcare professional
Meet the clinical threshold where a doctor would not be surprised if death occurs within 12 months
Conditions That May Qualify
The SR1 form is not limited to cancer. Patients with a wide range of conditions may qualify, including:
Advanced cancer
Organ failure (heart, lung, liver, kidney)
Neurological conditions (e.g. motor neurone disease, multiple sclerosis)
Advanced dementia
Severe frailty or complex comorbidities
Eligibility for an SR1 depends on the overall clinical picture, not just a specific diagnosis.
Important Clarifications
A patient does not need to be in their final days or weeks to qualify
Clinicians do not need to provide an exact life expectancy
If a patient lives longer than expected, there are no penalties for the clinician or the patient
Why This Matters for Care Providers
Care providers often see early signs of decline before a formal diagnosis reaches its final stage. You can:
Identify when a client’s condition becomes significantly progressive
Prompt timely conversations with healthcare professionals
Help families understand when an SR1 form may be appropriate
Recognizing eligibility early ensures clients receive financial support without unnecessary delays.
By understanding what is a SR1 form and who qualifies, care providers can act quickly and play a key role in securing timely support for vulnerable clients.
Who Can Complete an SR1 Form?
Only qualified healthcare professionals can complete an SR1 form. This ensures that the medical evidence used to fast-track benefit claims is accurate, credible, and accepted by the Department for Work and Pensions (DWP).
Healthcare Professionals Who Can Complete an SR1 Form
The following professionals can complete and submit an sr1 form:
Other registered clinicians with relevant expertise
The clinician must have sufficient knowledge of the patient’s condition to make an informed clinical judgment.
Who Cannot Complete an SR1 Form
Patients themselves
Family members or caregivers
Non-clinical staff
The sr1 form must always come from a recognised medical professional to be valid.
How Care Providers Should Work With Clinicians
Care providers do not complete the SR1 form, but they play an important supporting role:
Raise concerns early: Flag changes in a client’s condition to the GP or care team
Encourage timely action: Prompt families to request an SR1 when appropriate
Support communication: Share relevant observations that may help clinicians assess eligibility
Delays often happen because no one initiates the conversation with a clinician. Care providers are in a strong position to bridge that gap.
When care providers collaborate effectively with healthcare professionals, the SR1 form process starts earlier, helping clients access urgent financial support without delay.
Understanding who can complete an SR1 form UK helps you guide families correctly and ensures the process runs smoothly from the start.
You cannot download or request an SR1 form yourself. A healthcare professional must issue and complete it on your behalf. As a care provider, you can guide families through the correct steps to avoid delays.
Step-by-Step: How to Get an SR1 Form
Identify when the SR1 may be needed
Recognise signs of a progressive, life-limiting condition and raise this with the care team.
Speak to a healthcare professional
Ask the client’s GP, hospital consultant, or specialist nurse about completing an sr1 form.
Clinician assesses eligibility
The healthcare professional uses their judgment to decide if the patient meets the criteria.
The SR1 form is completed by the clinician
The clinician records diagnosis, progression, and relevant clinical details.
The form is submitted to the DWP
In most cases, the clinician sends the sr1 form directly.
Can You Download an SR1 Form?
The SR1 form download is not available to the public
Patients and families cannot access or complete the form themselves
Only authorised clinicians can request or generate the form
If a family asks for an SR1 form printable version, guide them to their GP or specialist instead of searching online.
How Care Providers Can Speed Up the Process
Act early when a client’s condition declines
Encourage families to request an SR1 during medical reviews
Follow up with clinicians if delays occur
The fastest way to secure an SR1 form UK is through direct communication with the patient’s healthcare team.
By understanding how to get an SR1 form, care providers can remove confusion, prevent unnecessary delays, and ensure clients access financial support as quickly as possible.
Can You Complete the SR1 Form Online?
Healthcare professionals can complete and submit the SR1 form online, but patients and families cannot access or fill it out themselves. The digital process is designed to speed up submissions and ensure secure handling of medical information.
How the SR1 Form Online Process Works
Clinicians request or access the form through secure NHS systems
They complete the SR1 form online using clinical details and professional judgment
The form is submitted directly to the Department for Work and Pensions (DWP) via secure channels
In many cases, digital submission replaces the need for postal forms, reducing delays and improving processing times.
NHS Systems Used for Submission
Healthcare professionals may use secure platforms such as:
NHS Spine (nhsspine)
NHS smartcard portal for authentication
Secure NHS email systems
These systems ensure that sensitive patient data is transmitted safely and efficiently.
The use of secure systems like the nhs spine allows clinicians to submit the SR1 form quickly, helping patients access urgent financial support without unnecessary delays.
What This Means for Care Providers
You do not need to handle or submit the form yourself
Your role is to ensure the right conversation happens with the clinician
Digital submission means faster turnaround for your clients
Encouraging clinicians to use the SR1 form online process can significantly reduce waiting times for benefit approvals.
Is There an SR1 Form Printable Version?
A sr1 form printable version exists for clinicians, but it is not publicly accessible
Most submissions now happen digitally due to speed and security advantages
By understanding how the SR1 form online process works, care providers can better support families and ensure no time is lost when urgent financial help is needed.
An SR1 form allows patients with a terminal illness to access certain UK benefits under special rules. These claims are prioritized, processed faster, and often awarded at the highest rate, making them essential for maintaining consistent care and financial stability.
Benefits That Accept an SR1 Form
A completed sr1 form UK can support fast-tracked claims for:
Personal Independence Payment (PIP)
Universal Credit (UC)
Employment and Support Allowance (ESA)
Disability Living Allowance (DLA) (for children)
Attendance Allowance (AA)
The sr1 form acts as medical evidence that allows these benefits to be processed under special rules for terminal illness.
What Changes When an SR1 Form Is Used
When a claim includes an SR1 form, the process becomes significantly easier:
No medical assessment required in most cases
Faster decision-making, often within days
Higher rate of payment, depending on the benefit
Why This Matters for Care Providers
Access to these benefits directly affects the level and continuity of care a client can receive. With faster approvals:
Clients can afford immediate care support
Families can reduce financial pressure during critical periods
Care providers can deliver consistent and uninterrupted services
The SR1 form bridges the gap between urgent care needs and financial support, ensuring that vulnerable clients receive help when it matters most.
Key Insight for Care Teams
Many families are unaware that these benefits can be fast-tracked. Care providers who understand what is an SR1 form can:
Educate families about available support
Encourage early application under special rules
Prevent delays that could impact care delivery
By knowing which benefits the SR1 form unlocks, care providers can play a proactive role in securing timely support for their clients.
Key Benefits of Using an SR1 Form
What is an SR1 Form
Using an SR1 form transforms how quickly and easily a patient can access financial support. For care providers, this directly impacts how fast care plans can be implemented and sustained.
1. No Medical Assessment Required
Patients supported by an sr1 form usually do not need to attend a face-to-face medical assessment. This removes delays and avoids unnecessary stress for individuals in a vulnerable condition.
2. Fast-Tracked Processing
Claims submitted with an SR1 form UK are prioritised by the Department for Work and Pensions (DWP).
Decisions are often made within days, not weeks
Urgent financial support becomes available much sooner
The sr1 form ensures that time-sensitive cases receive immediate attention.
3. Higher Rate of Payments
Most claims supported by an SR1 form qualify for the enhanced or highest rate of benefits.
This allows patients to:
Cover increased care costs
Access specialist support
Maintain quality of life
4. Reduced Administrative Burden
The sr1 simplifies the claims process:
Less paperwork compared to standard applications
Fewer follow-ups required
Minimal back-and-forth with assessors
Why This Matters for Care Providers
When a client uses an SR1 form, everything moves faster:
Care packages can start immediately
Funding gaps are reduced
Families gain peace of mind
The SR1 form is not just a document; it is a critical tool that enables timely care, financial stability, and better outcomes for patients and their families.
Understanding these benefits allows care providers to act quickly and ensure no client misses out on essential support.
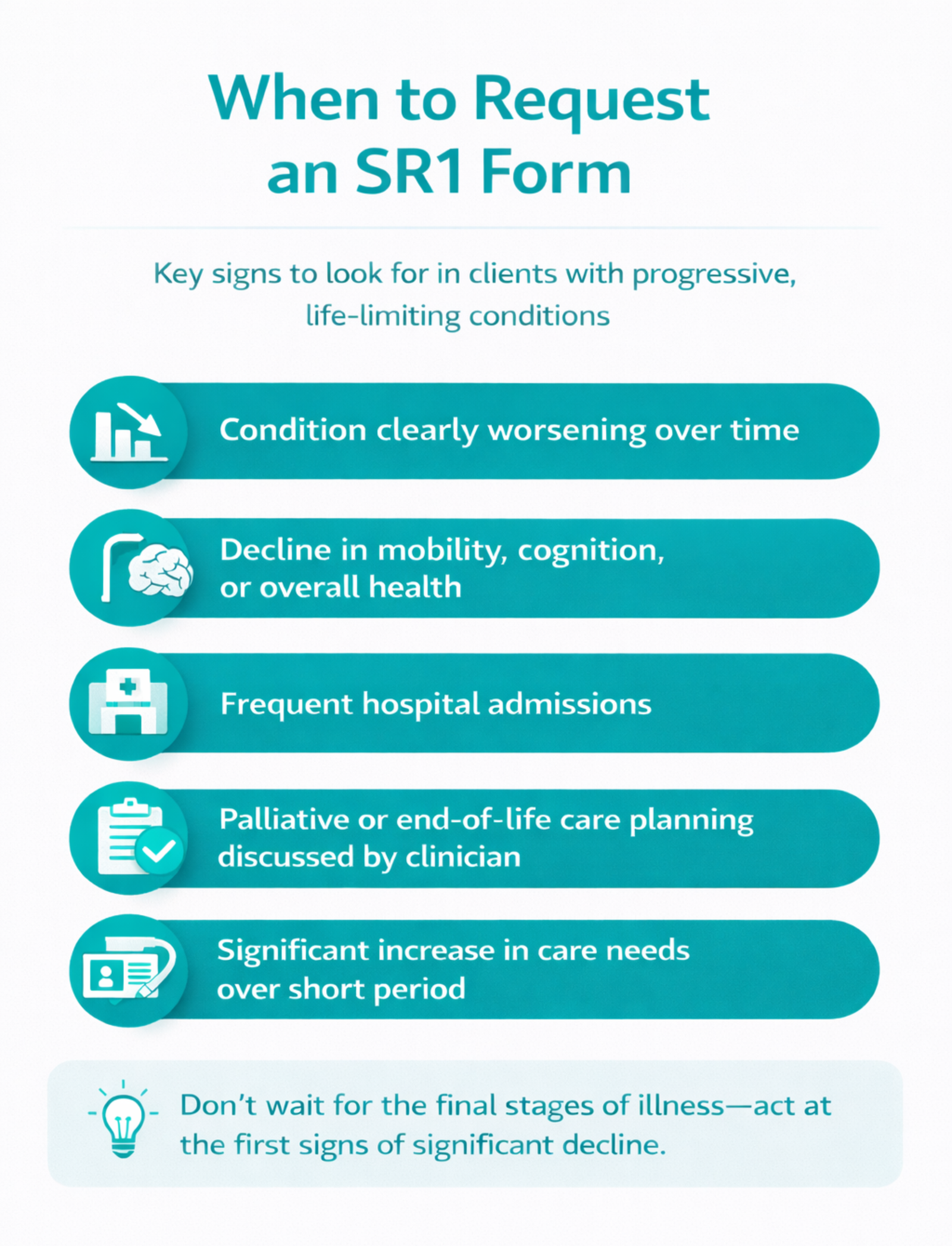
Care providers should raise the need for an SR1 form as soon as a client shows signs of a progressive, life-limiting condition. Acting early ensures the client can access fast-tracked financial support without delays.
Key Moments to Consider an SR1 Form
You should prompt a conversation about the sr1 form when:
A client’s condition is clearly worsening over time
There is a noticeable decline in mobility, cognition, or overall health
Hospital admissions become more frequent
A clinician discusses palliative or end-of-life care planning
Care needs increase significantly within a short period
Do not wait for the final stages of illness. The SR1 form applies earlier than many people realise.
Why Timing Matters
Delaying the sr1 form UK process can lead to:
Gaps in funding for care services
Increased stress for families
Delayed access to enhanced benefits
Starting early allows:
Faster approvals
Smoother care planning
Better support for both clients and families
How Care Providers Can Take Action
Observe and document changes in the client’s condition
Communicate concerns to the GP or care team promptly
Encourage families to request an SR1 during medical reviews
Follow up if the process is delayed
Expert Insight
Care providers often spend the most time with clients. Your observations can trigger the SR1 form process at the right time, ensuring clients receive the support they need without unnecessary waiting.
By recognising the right moment to request an SR1 form, care providers can take a proactive role in improving outcomes and ensuring timely access to essential benefits.
Common Mistakes Care Providers Should Avoid
Even when care providers understand the SR1 form, small mistakes can delay access to urgent financial support. Avoiding these errors ensures clients receive benefits quickly and without complications.
1. Waiting Too Long to Raise the SR1 Form
Many providers assume the sr1 form only applies in the final days or weeks of life. This is incorrect.
The criteria focus on a progressive condition, not exact timing
Delaying the conversation can slow down access to benefits
Raise the possibility of an SR1 form as soon as a client’s condition shows significant decline.
2. Assuming Only Cancer Patients Qualify
The SR1 form UK applies to a wide range of conditions, including:
Organ failure
Neurological diseases
Advanced dementia
Complex frailty
Limiting it to cancer cases prevents eligible clients from receiving support.
3. Not Communicating with Clinicians Early
Care providers often notice changes first, but delays happen when:
No one informs the GP or specialist
Families are unsure how to start the process
Early communication with healthcare professionals speeds up the sr1 process significantly.
4. Expecting Families to Handle Everything Alone
Families may not understand:
What an SR1 form is
How to request it
Why it matters
Care providers should guide them clearly and confidently.
5. Misunderstanding the Process
Common misconceptions include:
Believing patients can complete the sr1 form themselves
Thinking a formal prognosis is required
Assuming there are penalties if a patient lives longer than expected
These misunderstandings can create unnecessary delays or hesitation.
Why Avoiding These Mistakes Matters
Mistakes in the SR1 form process can:
Delay benefit approvals
Interrupt care services
Increase stress for families
Getting the SR1 form process right the first time ensures clients receive fast, reliable support when they need it most.
By avoiding these common pitfalls, care providers strengthen their role as trusted advisors and improve outcomes for the people they support.
An SR1 form is a clinical document, not a detailed medical report. It focuses on key information that allows the Department for Work and Pensions (DWP) to quickly confirm eligibility under special rules.
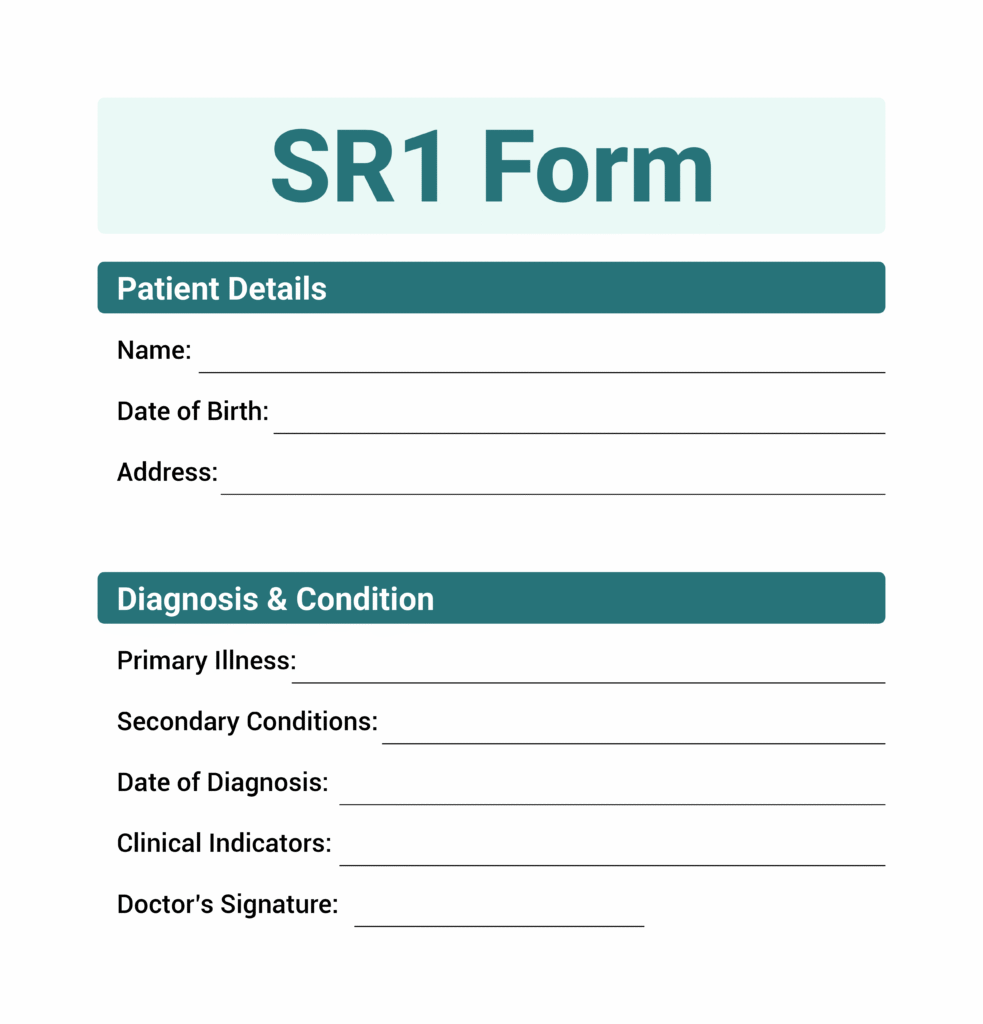
SR1 Form Example: Core Information Included
A typical sr1 form example will include:
Patient details
Name, date of birth, and address
Diagnosis and condition
Primary illness and any relevant secondary conditions
Date of diagnosis
When the condition was first identified
Clinical indicators
Evidence that the condition is progressive and life-limiting
Awareness of condition
Whether the patient understands their diagnosis and prognosis
Treatment plan
Current or planned care approach
Clinician details
Name, role, registration number, and organisation
How Clinicians Complete the SR1 Form
Healthcare professionals complete the SR1 form using clear clinical language. They do not need to:
Provide an exact life expectancy
Write lengthy explanations
Include unnecessary medical history
The goal of the sr1 form is to confirm eligibility quickly, not to produce a full medical assessment.
What Care Providers Should Know
Care providers do not complete the SR1 form, but understanding its structure helps you:
Explain the process confidently to families
Prepare relevant information for discussions with clinicians
Ensure nothing delays submission
Important Note
There is no publicly available SR1 form printable or editable version for patients
Only authorised clinicians can access and complete the official form
Understanding a basic SR1 form example helps care providers support the process more effectively and avoid confusion.
By knowing what information the SR1 form requires, care providers can play a proactive role in ensuring timely and accurate submissions.
Final Thoughts…
The SR1 form is one of the most important tools available to support clients with life-limiting conditions. It enables fast access to financial support, removes unnecessary assessments, and ensures care can continue without interruption.
As a care provider, you are often the first to recognise when a client’s condition is declining. Acting on that insight, by encouraging an SR1 form request at the right time, can make a significant difference to both the client and their family.
What Care Providers Should Remember
Act early when a condition becomes progressive
Guide families clearly through the SR1 form UK process
Communicate effectively with healthcare professionals
Avoid delays by addressing eligibility as soon as possible
The SR1 form is not just paperwork; it is a gateway to timely support, dignity, and better care outcomes.
By understanding what is an SR1 form and using that knowledge in practice, care providers position themselves as trusted partners in both care delivery and client advocacy.
Need Help Navigating SR1 Forms and Care Compliance?
At Care Sync Experts, we support care providers in handling critical processes like the SR1 form with clarity, speed, and confidence.
Whether you need help with:
Understanding when to request an SR1 form for your clients
Supporting families through fast-tracked benefit applications
Ensuring compliance with CQC and care regulations
Strengthening your care operations and documentation
Preparing your business for growth, contracts, and inspections
We’re here to guide you every step of the way.
Don’t let delays in the SR1 form UK process affect your clients’ access to essential support.
Let our experts simplify the process so you can focus on delivering high-quality care.
Book a consultation with Care Sync Experts and ensure your care business is equipped to support clients when it matters most.
FAQ
What is a S1 form in the UK?
The S1 form is different from the SR1 form. It is used for healthcare access, not benefits. An S1 form allows UK nationals living in another European country (or vice versa) to access state healthcare funded by the UK. It has no connection to terminal illness benefit claims.
How much is terminal illness benefit in the UK?
There is no single “terminal illness benefit.” Instead, individuals receive fast-tracked access to existing benefits (such as PIP, UC, ESA, or Attendance Allowance). In most cases, claims supported under special rules qualify for the highest rate, which can range from around £72 to over £180 per week depending on the benefit.
How do I apply for Attendance Allowance in England?
To apply for Attendance Allowance, you must: – Request or download the claim form from GOV.UK or by phone – Complete the form with details about care needs – Indicate if you are applying under special rules for terminal illness – Ask a healthcare professional to complete an SR1 form – Submit the application by post
Claims supported by an SR1 form are processed faster and usually awarded at the higher rate.
How much is full Attendance Allowance in the UK?
As of current UK rates, the higher rate of Attendance Allowance is approximately £108.55 per week (subject to annual updates). People who apply under special rules for terminal illness are typically awarded this higher rate automatically.
The Health and Safety at Work Act 1974 (HASAWA) is the primary UK law that requires employers to protect the health, safety, and welfare of employees and anyone affected by their work.
It applies to most workplaces, including care homes and domiciliary care services, and places legal responsibility on those who create risks to manage them.
In simple terms, the HASAWA meaning is this: if you run a care business, you must take all reasonably practicable steps to keep your staff, patients, and the public safe at all times.
The health & safety at work act directly affects how caregiver businesses operate every day. Care providers work in high-risk environments where staff support vulnerable people, handle medication, and perform physical tasks like lifting and moving patients. Without strong safety practices, both carers and service users face serious harm.
The health and safety act 1974 ensures care businesses build safe systems of work. For example, a domiciliary care agency must train staff on safe manual handling to prevent injuries when assisting clients. A care home must control infection risks to protect residents and staff. These are not optional practices, they are legal duties under hasawa health and safety at work act.
In real terms, this law helps care providers:
Reduce staff injuries from lifting, slips, and fatigue
Protect patients from unsafe care practices
Maintain compliance required for CQC inspections
Avoid incidents that could lead to service closure or legal action
For caregiver businesses, the Act is not just a legal requirement—it is the foundation of safe, high-quality care.
Health and Safety at Work Act 1974 Employers Responsibilities
The Health and Safety at Work Act 1974 employers responsibilities require care providers to actively protect staff, patients, and anyone affected by their services. Employers must not wait for incidents to happen; they must prevent risks before harm occurs.
In a caregiver business, this means putting clear systems, training, and safeguards in place every day.
Key Employer Duties Under HASAWA
Provide a safe working environment
Employers must maintain clean, hazard-free care settings, whether in care homes or clients’ homes.
Ensure safe equipment and systems of work
Care providers must supply and maintain equipment such as hoists, PPE, and medical tools, and ensure staff use them correctly.
Carry out risk assessments
Employers must identify risks (e.g. manual handling, infection, medication errors) and take action to control them.
Deliver proper training and supervision
Staff must receive training in areas like safeguarding, moving and handling, and infection control to work safely.
Provide adequate welfare facilities
This includes access to rest areas, hygiene facilities, and support systems for staff wellbeing.
Create and maintain a health and safety policy
Businesses with five or more employees must document how they manage health and safety and communicate it clearly to staff.
What This Means in Practice
A care provider must ensure carers know how to safely lift a client, use protective equipment correctly, and respond to emergencies. If an employer fails to provide training or safe systems, they breach the health and safety policy requirements and risk enforcement action.
In short, employers carry the primary responsibility for creating a safe care environment under the health and safety at work act 1974.
Health and Safety at Work Act 1974 Section 2 Explained
Duties of Employers HASAWA
Section 2 of the Health and Safety at Work Act 1974 sets out the core duty of employers: they must protect the health, safety, and welfare of employees while they are at work.
In simple terms, Health and Safety at Work Act 1974 Section 2 means employers must take practical steps to prevent harm, not just react when something goes wrong.
What Section 2 Requires from Care Providers
Section 2 focuses on five key areas:
Safe systems of work
Care providers must design tasks so staff can work safely—for example, using proper moving and handling procedures when assisting patients.
Safe use, handling, and storage of equipment and substances
This includes safely managing medications, cleaning chemicals, and medical devices.
Adequate training, instruction, and supervision
Employers must ensure carers understand risks and know how to perform their duties safely.
Safe workplace environment
Care settings must be free from hazards such as slippery floors, faulty equipment, or unsafe layouts.
Welfare provisions
Employers must provide facilities that support staff wellbeing, such as rest areas, clean washing facilities, and access to drinking water.
What This Means in a Care Setting
For example, a domiciliary care agency must train carers on how to safely support a client with limited mobility. A care home must ensure staff follow infection control procedures when handling residents or equipment.
If an employer ignores these responsibilities, they breach Section 2, which can lead to enforcement action by regulators.
In practice, Section 2 forms the backbone of how caregiver businesses deliver safe, compliant, and high-quality care every day.
Who is Responsible for Health and Safety in the Workplace?
Many care providers ask: Who is responsible for health and safety in the workplace?
The Health and Safety at Work Act 1974 makes this clear—responsibility is shared, but employers carry the primary duty.
Employer Responsibility
Employers hold the main legal responsibility under the health and safety act 1974. They must:
Create safe systems of work
Provide training, equipment, and supervision
Carry out risk assessments
Protect both staff and service users
In a care business, this means ensuring carers can safely support clients, manage risks in home environments, and follow proper procedures at all times.
Employee Responsibility
Employees also have legal duties. Under HASAWA, they must:
Take reasonable care of their own safety and others
Follow training and workplace procedures
Use equipment correctly (e.g. PPE, hoists)
Report hazards, incidents, or unsafe conditions
For example, a carer must report a faulty hoist instead of continuing to use it.
Manager and Supervisor Responsibility
Managers act on behalf of the employer and must:
Enforce safety procedures
Monitor staff performance
Address risks quickly
Ensure compliance with policies
The Key Principle
According to the health and safety at Work Act 1974, who is responsible for health and safety at Work?
Everyone has a role, but employers are ultimately accountable.
In caregiver businesses, strong teamwork between employers, managers, and staff ensures a safe environment for both carers and vulnerable service users.
HSE stands for the Health and Safety Executive. It is the UK government body responsible for enforcing the Health and Safety at Work Act 1974 and ensuring workplaces operate safely.
What the HSE Does
The HSE regulates and monitors how businesses manage health and safety. In caregiver settings, this includes:
Inspecting workplaces
HSE inspectors visit care providers to check compliance with safety laws and procedures.
Investigating incidents
They investigate serious accidents, injuries, or unsafe practices in care environments.
Enforcing the law
The HSE can issue improvement notices, prohibition notices, fines, or even prosecute businesses that fail to meet safety standards.
Providing guidance
They publish practical guidance to help employers understand and meet their legal duties.
HSE and Care Providers
For care businesses, the HSE works alongside regulators like the CQC. While the CQC focuses on care quality, the HSE focuses specifically on health and safety risks, such as staff injuries, unsafe equipment, or poor working conditions.
If a care provider ignores safety responsibilities, the HSE can take immediate action to protect workers and the public. This makes compliance with the health and safety at work act 1974 not just important, but essential for staying operational.
How the Management of Health and Safety at Work Regulations 1999 Supports HASAWA
The Management of Health and Safety at Work Regulations 1999 builds on the Health and Safety at Work Act 1974 by focusing on how businesses manage risks in practice.
While HASAWA sets the legal duty, these regulations explain how to carry it out day-to-day.
What These Regulations Require
Care providers must:
Carry out risk assessments
Identify hazards in care settings, such as manual handling risks, infection exposure, or unsafe home environments.
Implement control measures
Take action to reduce or eliminate risks, for example, using hoists, PPE, or safer care plans.
Appoint competent persons
Assign trained individuals to manage health and safety within the organisation.
Provide clear procedures
Ensure staff know what to do in emergencies, such as falls, medication errors, or safeguarding concerns.
Protect vulnerable people
Consider risks to both staff and service users, especially those with higher care needs.
What This Means for Caregiver Businesses
In practice, a care provider cannot rely on policies alone. They must actively assess each situation, whether in a care home or a client’s house, and adapt safety measures accordingly.
For example:
Before lifting a client, a risk assessment must confirm the safest method
Before administering medication, staff must follow clear safety procedures
Before entering a client’s home, carers must identify environmental risks
The Key Difference
The health and safety at work act 1974 sets the duty
The Management of Health and Safety at Work Regulations 1999 ensures the duty is properly managed
Together, they form the backbone of effective safety systems in caregiver businesses.
Failing to follow the Health and Safety at Work Act 1974 puts care providers at serious legal, financial, and operational risk. Regulators do not overlook breaches, especially in environments where vulnerable people depend on safe care.
Legal Consequences
If a care business fails to meet its duties under the health and safety act 1974, enforcement bodies like the HSE can:
Issue prohibition notices to stop unsafe activities instantly
Impose fines or prosecute the business and its directors
In severe cases, pursue criminal charges
Impact on Care Operations
Non-compliance does not just lead to legal action—it disrupts the entire business:
Service suspension or closure
Unsafe care environments can lead to immediate shutdowns.
Failed inspections (CQC impact)
Poor safety practices often result in lower inspection ratings.
Loss of contracts
Local authorities and the NHS avoid working with non-compliant providers.
Reputational damage
Negative reports reduce trust from families, commissioners, and staff.
Real Risk in Care Settings
In caregiver businesses, safety failures can lead to:
Staff injuries from unsafe lifting practices
Medication errors due to poor procedures
Infection outbreaks from weak controls
Harm to vulnerable service users
The health & safety act 1974 is not just a legal framework; it protects lives. Care providers who ignore their responsibilities risk losing their business, their reputation, and most importantly, the safety of the people they serve.
Health and Safety Checklist for Caregiver Businesses
Health and safety at work legislation
Care providers must apply the Health and Safety at Work Act 1974 in daily operations—not just in policy documents. Use this checklist to stay compliant and protect both staff and service users.
Practical Health and Safety Checklist
Carry out regular risk assessments
Assess risks in care homes and clients’ homes, including manual handling, infection control, and environmental hazards.
Maintain a clear health and safety policy
Document how your organisation manages risks and ensure all staff understand it.
Provide ongoing staff training
Train carers on moving and handling, safeguarding, medication safety, and emergency procedures.
Supply and maintain safe equipment
Ensure hoists, PPE, and medical tools are safe, regularly checked, and used correctly.
Monitor staff compliance
Supervisors must check that staff follow procedures and apply training in real situations.
Report and record incidents properly
Log accidents, near misses, and risks to improve safety and meet legal requirements.
Ensure proper supervision and support
Provide guidance to staff, especially when handling complex care situations.
Review and update procedures regularly
Adapt safety measures based on new risks, feedback, or regulatory updates.
Following this checklist helps care providers meet their duties under the health & safety at work act, avoid enforcement action, and deliver safe, high-quality care consistently.
In caregiver businesses, strong safety practices are not optional—they are essential for protecting lives and maintaining trust.
Final Thoughts…
The Health and Safety at Work Act 1974 is more than a legal requirement—it is the foundation of safe, reliable care delivery. For caregiver businesses, it defines how you protect your staff, your service users, and your reputation.
At its core, the health and safety act 1974 places responsibility on those who create risks to manage them. This means care providers must take proactive steps every day—through training, supervision, risk assessments, and clear procedures—to prevent harm before it happens.
Understanding what the health and safety at work act is helps care businesses move beyond compliance and build safer, more efficient operations. Whether you run a care home or a domiciliary care service, applying these principles strengthens your ability to pass inspections, win contracts, and deliver high-quality care.
In simple terms: – Safe care is not optional – Compliance is not a one-time task – Responsibility sits with everyone, but starts with the employer
Care providers who take the health & safety act 1974 seriously do more than follow the law, they create environments where both carers and service users can thrive safely.
Need Help with DBS Compliance or Care Business Setup?
At Care Sync Experts, we help care providers stay compliant, win contracts, and grow with confidence.
Whether you need support with:
Enhanced DBS processes and safeguarding compliance
CQC registration and inspection readiness
Tender writing and contract acquisition
Policies, documentation, and operational setup
We’ve got you covered.
Don’t risk delays, failed inspections, or lost opportunities. Let our experts handle the complexity so you can focus on delivering quality care.
Book a consultation with Care Sync Experts and take the next step toward building a compliant, scalable care business.
FAQ
What law regulates health and safety in the workplace?
The Health and Safety at Work Act 1974 is the main law that regulates workplace health and safety in the UK. It sets the legal duties for employers and employees and is supported by additional regulations, such as the Management of Health and Safety at Work Regulations 1999, which focus on risk assessments and day-to-day safety management.
What is health and safety?
Health and safety refers to the systems, procedures, and actions put in place to prevent injury, illness, and harm in the workplace. In care settings, this includes safe patient handling, infection control, proper use of equipment, and protecting both staff and service users from risks.
Why is health and safety important in the workplace?
Health and safety is important because it protects lives, reduces workplace injuries, and ensures businesses operate legally. In caregiver businesses, strong safety practices prevent harm to vulnerable service users, reduce staff injuries, and improve overall care quality.
What is a risk in health and safety?
A risk in health and safety is the chance that a hazard could cause harm. For example, lifting a patient without proper equipment creates a risk of injury to both the carer and the service user. Care providers must identify these risks and take steps to control or eliminate them.
New Style Jobseeker’s Allowance (JSA) pays up to £72.90 per week if you’re under 25 and up to £92.05 per week if you’re 25 or over in the 2025/26 tax year. You can usually receive this JSA payment for up to 182 days (about 6 months) while you actively look for work.
JSA is not means tested, so your savings or your partner’s income do not affect your claim. Instead, eligibility depends on your National Insurance contributions, making it different from other unemployment and benefits support.
In short, if you’re asking how much is JSA or how much is job seekers allowance, the answer depends mainly on your age and contribution history, not your savings.
You usually receive JSA every 2 weeks into your bank account
Duration:
You can claim for up to 182 days (around 6 months)
Means testing:
New Style JSA is not means tested, so savings and partner income do not affect your claim
Eligibility basis:
Your entitlement depends on your National Insurance contributions, not household finances
Work requirement:
You must be actively looking for work and meet your Jobcentre agreement
Other benefits:
You can sometimes claim JSA alongside Universal Credit, depending on your situation
If you’re wondering is job seekers allowance means tested, the answer for New Style JSA is no, but you must still meet strict JSA eligibility rules based on your work history.
What JSA Means for Care Workers and Care Providers
Jobseeker’s Allowance plays an important role in the care sector, where employment can be unpredictable. Many care workers move between roles, work on zero-hour contracts, or take short breaks between placements. During these periods, JSA provides short-term financial support while they look for new work.
For care workers, JSA helps bridge gaps between jobs without relying entirely on savings. Since New Style JSA is not means tested, workers can still receive support even if they have some savings or a working partner. This makes it a useful option for those navigating unemployment and benefits in a sector with fluctuating hours.
For care providers, JSA indirectly supports workforce stability. When staff leave or contracts end, access to JSA allows workers to remain financially secure while searching for their next role, often within the same sector. This reduces long-term workforce loss and helps agencies rehire experienced carers more easily.
In practical terms, JSA functions as a form of short-term unemployment insurance, giving both workers and employers breathing room during transitions. For providers facing staffing shortages, understanding how JSA works can also help when advising candidates or supporting staff between roles.
JSA Eligibility: Who Can Claim Job Seeker’s Allowance?
To claim Job Seekers Allowance, you must meet specific conditions based on your work history and availability for work. New Style JSA focuses on contributions, not your financial situation.
Basic JSA eligibility requirements:
You can claim if you:
Are 18 or over and below State Pension age
Live in Great Britain
Have paid Class 1 National Insurance contributions in the last 2–3 years
Work less than 16 hours per week
Are available for work and actively looking for a job
Who cannot claim JSA?
You will not qualify if:
You work 16 hours or more per week
You cannot work due to illness or disability (you may need ESA instead)
You have not built enough National Insurance contributions
Care sector example:
A care worker who recently left a domiciliary care role and has been paying National Insurance can usually claim JSA while searching for a new position, especially if they are working reduced hours or between contracts.
If you want to claim job seekers allowance, focus on your work history and job search activity. Your savings or household income will not stop you from qualifying under New Style JSA eligibility rules.
Can I Claim Job Seekers Allowance If I Have Savings?
Yes, you can claim Job Seekers Allowance if you have savings when applying for New Style JSA.
New Style JSA is not means tested, which means:
Your savings do not affect your claim
Your partner’s income or savings do not affect your claim
You can still qualify even if you have money in the bank
This directly answers the common question: “Can I claim job seekers allowance if I have savings?” → Yes, you can.
Why savings don’t matter
New Style JSA works differently from older benefits. Instead of assessing your finances, it looks at your National Insurance contributions.
If you have worked and paid enough contributions in recent years, you may qualify regardless of how much you have saved.
Important exception to understand
If you apply for Universal Credit instead, your savings will be assessed
If you receive older income-based JSA, savings may also affect eligibility
Care sector example
A care worker who has saved money while working in a care home can still claim JSA after leaving their job. Even with savings, they can receive support while applying for new roles.
So if you’re asking:
“Is job seekers allowance means tested?” → Not for New Style JSA
“Can I claim job seekers allowance if I have savings?” → Yes, as long as you meet contribution-based requirements
How Much Is Job Seekers Allowance Per Week and Month?
JSA vs Universal Credit
The amount you receive depends mainly on your age. New Style JSA sets a maximum weekly payment, but your actual amount may be lower in some cases.
Weekly JSA payment rates (2025/26):
£72.90 per week if you are aged 18–24
£92.05 per week if you are 25 or over
How much is Job Seekers Allowance a month?
Although JSA is paid weekly, you can estimate the monthly amount:
Under 25: about £291 per month
25 or over: about £368 per month
This answers common searches like:
how much is job seekers allowance a month
jobseekers how much
What can affect your JSA payment?
You may receive less than the maximum if:
You work part-time
You receive a pension or other income
You do not fully meet your job search requirements
Using a Job Seekers Allowance calculator
A job seekers allowance calculator can help you estimate your exact payment based on your situation. However, for New Style JSA, the calculation is usually straightforward since it depends mostly on:
Your age
Your National Insurance contributions
Care sector example
A care assistant aged 30 who recently left a role can receive up to £92.05 per week while searching for a new job. If they take on a few part-time shifts, their JSA payment may reduce slightly depending on earnings.
In simple terms, if you’re asking how much is job seekers allowance, most people receive between £72.90 and £92.05 per week, depending on age and circumstances.
How Long Can You Claim Job Seekers Allowance?
You can usually claim New Style Jobseeker’s Allowance for up to 182 days, which is about 6 months.
This directly answers the question: “How long can you claim job seekers allowance?” → Up to 6 months in most cases.
What happens after 6 months?
Once your JSA ends, you have a few options:
Apply for Universal Credit if you still need financial support
Continue working with your Jobcentre work coach to find employment
Explore training or alternative benefits depending on your situation
Important to know
JSA does not renew automatically after 182 days
You must continue to meet job search requirements throughout your claim
Missing commitments can lead to your payments being reduced or stopped
Care sector example
A care worker between roles may claim JSA while applying for new positions in domiciliary care or care homes. If they do not secure a job within 6 months, they may transition to Universal Credit while continuing their job search.
In simple terms, JSA provides short-term support, not long-term income. It helps you stay financially stable while actively looking for your next job.
How to Apply for JSA (Step-by-Step)
If you want to apply for JSA, the process is straightforward, but you must follow each step carefully to avoid delays.
Step 1: Start your JSA application
You can apply online through GOV.UK. This is the fastest way to begin your claim.
This answers common searches like:
job seekers allowance apply
jsa applications
how do I get Job Seekers Allowance
Step 2: Prepare your details
Before you apply, gather:
Your National Insurance number
Your bank account details
Your employment history (last 6 months)
Details of any income or part-time work
Having this ready speeds up your application.
Step 3: Attend your Jobcentre interview
After submitting your application, the Jobcentre will invite you to an interview.
During this meeting, you will:
Confirm your details
Discuss your job search
Agree to a Claimant Commitment
This agreement outlines how you will actively look for work.
Step 4: Start receiving payments
You may wait up to 7 days before your claim starts
Your first payment may take up to 2 weeks
After that, you will receive JSA payment every 2 weeks
Important rules during your claim
To continue receiving JSA, you must:
Actively apply for jobs
Attend scheduled Jobcentre meetings
Follow your Claimant Commitment
If you fail to meet these conditions, your payments may be reduced or stopped.
Care sector example
A care assistant who recently left a role can claim job seekers allowance online, attend a Jobcentre interview, and begin receiving payments while applying for new care jobs.
In simple terms, to claim job seekers allowance, apply online, attend your interview, and actively search for work to keep receiving payments.
JSA Contact Number and Support
If you need help with your claim, you can contact Jobcentre Plus, which handles all JSA enquiries.
Job Seekers Allowance contact telephone number
Telephone: 0800 055 6688
Opening hours: Monday to Friday, usually 8am to 5pm
Calls are free from mobiles and landlines
This covers common searches like:
job seekers allowance contact telephone number
jsa contact no
jsa enquiries number
jsa allowance contact number
When should you call?
You should contact Jobcentre Plus if:
You need help with your JSA application
You want to check your claim status
You need to report a change in circumstances
You missed an appointment or payment
What to prepare before calling
To avoid delays, have the following ready:
Your National Insurance number
Your personal details (name, address)
Details of your claim or application
Alternative support options
Visit your local Jobcentre Plus office
Request help if English is not your first language
Ask for support with online applications if needed
Care sector tip
Care workers moving between jobs often need quick support to keep their claims active. Calling early and keeping records of conversations can help avoid payment issues during job transitions.
If you’re unsure about your claim, using the JSA contact number is the fastest way to get direct support and resolve issues quickly.
Job Seekers Allowance Rules You Must Follow
Types of Employee Benefits
To keep receiving JSA, you must follow strict job seekers allowance rules set by the Department for Work and Pensions (DWP). These rules focus on your commitment to finding work.
Your main responsibilities
You must:
Actively search for work every week
Be available to start work immediately
Attend all Jobcentre appointments
Follow your agreed Claimant Commitment
Your Claimant Commitment outlines the steps you will take to find a job, such as applying for roles, attending interviews, or completing training.
What happens if you don’t follow the rules?
If you fail to meet these requirements:
Your JSA payment may be reduced or stopped
You may receive a sanction, which pauses your payments
You must provide a valid reason (for example, illness or emergencies) to avoid penalties
Understanding the 35-hour job search rule
Traditionally, claimants are expected to spend around 35 hours per week looking for work. However, policies can change, and there have been discussions around flexibility in job search expectations depending on individual circumstances.
If you’ve heard that the DWP is ending the 35-hour work search rule, it’s important to check with your work coach, as requirements can vary based on your situation.
Care sector example
A care worker claiming JSA may agree to:
Apply for a set number of care jobs weekly
Attend interviews with care agencies
Complete refresher training (e.g. safeguarding)
Failing to meet these commitments without a valid reason could result in reduced payments.
In simple terms, JSA is not automatic income. You must actively prove that you are looking for work and ready to return to employment.
How Care Providers Can Support Staff on JSA
Care providers play a key role in supporting staff who are between roles or experiencing reduced hours. Understanding how JSA works allows providers to guide workers through transitions and maintain a strong workforce.
1. Support staff during employment gaps
When a care worker leaves or finishes a contract, providers can:
Inform them about how to claim Job Seekers Allowance
Encourage early applications to avoid payment delays
Direct them to Jobcentre support services
This helps workers stay financially stable while searching for new roles.
2. Maintain a talent pipeline
Care providers can use JSA periods as an opportunity to:
Reconnect with experienced carers
Offer flexible or part-time roles
Build a pool of workers ready to return quickly
Workers receiving JSA often remain active job seekers, making them ideal candidates for rapid recruitment.
3. Provide guidance on compliance
Providers can help staff understand:
JSA eligibility requirements
Job search expectations
How part-time work affects their JSA payment
Clear guidance reduces confusion and helps workers avoid sanctions.
4. Encourage training and upskilling
During periods of unemployment, providers can:
Recommend short courses (e.g. care certifications)
Support refresher training
Prepare staff for higher-level roles
This improves both worker confidence and service quality.
5. Strengthen retention and reputation
When providers support staff even after contracts end, they:
Build trust and loyalty
Increase the likelihood of staff returning
Enhance their reputation as a supportive employer
Care sector insight
Many care workers move between roles due to the nature of the industry. Providers who understand unemployment and benefits systems like JSA can better support staff transitions and reduce long-term workforce shortages.
In simple terms, JSA is not just a worker benefit, it is also a tool that care providers can use to retain talent, support staff, and strengthen recruitment pipelines.
Conclusion
Jobseeker’s Allowance offers short-term financial support while you actively look for work. If you meet the JSA eligibility requirements, you can receive up to £72.90 or £92.05 per week, depending on your age, for up to 6 months.
For care workers, JSA helps bridge employment gaps between roles. For care providers, it supports workforce stability by keeping skilled workers active in the job market.
If you’re considering your options:
Check your eligibility early
Start your JSA application as soon as your work situation changes
Stay consistent with your job search requirements
Explore Universal Credit if you need longer-term support
If you’re asking “how much is JSA”, the real value goes beyond the weekly payment. JSA gives you time, stability, and support while you secure your next role, especially in fast-moving sectors like care.
Need Support Navigating Compliance, Staffing, or Care Business Growth?
At Care Sync Experts, we help care providers stay compliant, strengthen their workforce, and grow with confidence.
Whether you need support with:
CQC registration and inspection readiness
Staff compliance, onboarding, and retention strategies
Tender writing and securing local authority contracts
Policies, documentation, and operational setup
We’ve got you covered.
Don’t let staffing gaps, compliance issues, or missed opportunities slow your growth.
Let our experts handle the complexity while you focus on delivering high-quality care.
Book a consultation with Care Sync Experts and take the next step toward building a compliant, scalable, and resilient care business.
FAQ
What are the two types of JSA?
There are two main types of Jobseeker’s Allowance in the UK: – New Style JSA – based on your National Insurance contributions and not means tested – Income-based JSA – an older benefit that is now being replaced by Universal Credit and is no longer available for new claims
Most new applicants will apply for New Style JSA, sometimes alongside Universal Credit.
Can I claim JSA if I have redundancy pay?
Yes, you can still claim New Style JSA if you have redundancy pay. Redundancy payments do not usually affect your eligibility because New Style JSA is based on your National Insurance contributions, not your savings or lump-sum payments. However, if you apply for Universal Credit, your redundancy pay may be taken into account.
Can I claim JSA if I resign?
You can claim JSA if you resign, but your payments may be delayed or reduced. The Jobcentre will assess your reason for leaving. If they decide you left your job without a good reason, you may receive a sanction, which means your payments could be paused for a period of time. Valid reasons may include workplace issues, health concerns, or unsafe working conditions.
What proof do I need for New Style JSA?
To apply for New Style JSA, you typically need to provide: – Your National Insurance number – Proof of identity (such as passport or driving licence) – Details of your recent employment history – Your bank account details – Information about any income or part-time work
The Jobcentre may also ask for additional documents during your application or interview.
An enhanced DBS CRB check is the highest level of background check carried out by the UK’s Disclosure and Barring Service. It shows spent and unspent convictions, cautions, local police intelligence, and barred list status for people working with children or vulnerable adults. Employers must request this check for regulated roles such as caregivers, nurses, and support workers.
An enhanced DBS check typically costs £49.50 (excluding any service fees) and takes 7 to 14 days to complete, although delays can occur if multiple police forces need to review the application. This check plays a critical role in safeguarding, making it a legal and operational requirement for most care providers.
An enhanced DBS CRB check is the highest level of criminal record check in the UK
It includes convictions, cautions, police intelligence, and barred lists
Caregivers and healthcare staff must pass this check to work in regulated roles
Employers (not individuals alone) must initiate the application
The standard fee is £49.50, and results usually arrive within 7–14 days
There is no official expiry, but employers often request renewal every 1–3 years
What Is an Enhanced DBS CRB Check?
An enhanced DBS CRB check is a safeguarding requirement that allows care providers to verify whether a person is safe to work with vulnerable individuals. If you run a care agency, manage a care home, or recruit support staff, this check protects your clients, your business, and your regulatory standing.
In simple terms, what is a DBS check?
A DBS check is a background screening process carried out by the Disclosure and Barring Service to review a person’s criminal record and suitability for specific roles. The enhanced CRB DBS version goes further than a basic DBS check by including sensitive information relevant to safeguarding.
From a caregiver business standpoint, this is not optional; it is a core compliance requirement.
Why It Matters in Care Services
Protects vulnerable people: You ensure that staff working with children, elderly individuals, or people with disabilities are safe and suitable
Supports regulatory compliance: Regulators like CQC expect strict DBS checks as part of safe recruitment practices
Improves trust and reputation: Families and commissioners trust providers who follow proper safeguarding procedures
Reduces legal risk: Hiring without proper checks can lead to serious legal and operational consequences
Enhanced vs Basic DBS Check (Quick Context)
A basic DBS check only shows unspent convictions.
An enhanced DBS CRB check provides a full safeguarding picture, which makes it essential for caregiver roles.
If you employ or manage caregivers, you must treat DBS checks as part of your standard hiring process, not an afterthought.
Care providers must follow strict enhanced DBS CRB requirements when hiring staff. If a role involves direct contact with vulnerable people, you must request an enhanced DBS check before allowing the person to start work.
Roles That Require an Enhanced DBS Check
In the care sector, you must carry out an enhanced DBS check for:
Care workers and domiciliary caregivers
Support workers and healthcare assistants
Nurses and clinical staff
Care home managers and supervisors
Agency staff working with vulnerable adults or children
Volunteers involved in regulated care activities
If your staff provide personal care, handle medication, or support daily living, the role almost always falls under regulated activity.
What Counts as Regulated Activity?
A role qualifies as regulated activity if the worker:
Provides personal care (washing, dressing, feeding)
Supports individuals with healthcare or medication
Works closely with children or vulnerable adults on a regular basis
Has unsupervised access to people receiving care
If the answer is yes to any of the above, you must complete an enhanced DBS check.
Why This is Important for Care Providers
Regulators expect strict compliance with DBS requirements
Commissioners often require proof of DBS checks before awarding contracts
Failing to carry out checks can lead to serious legal consequences
If you run a care business, treat enhanced DBS checks as a non-negotiable hiring step.
What Does an Enhanced DBS Check Include? (CRB Checklist)
Different Levels of DBS Check
An enhanced DBS CRB check provides a complete safeguarding profile of an individual. As a care provider, you use this information to decide whether a candidate is safe to work with vulnerable people.
Here is a clear CRB checklist of what the enhanced check includes:
1. Criminal Record (Spent and Unspent)
The check shows:
Unspent convictions
Relevant spent convictions
Cautions, reprimands, and final warnings
This gives you a full history, not just recent offences.
2. Local Police Intelligence
Police forces may include additional information they believe is relevant to the role.
This may not appear on standard checks
It helps identify potential risks that are not captured in convictions
This is one of the key reasons the enhanced CRB DBS is required in care roles.
3. Barred Lists Check
The enhanced DBS check can confirm if a person is:
Barred from working with children
Barred from working with vulnerable adults
Or both (depending on the role)
If someone appears on a barred list, you must not employ them in regulated activity.
4. Identity and Eligibility Verification
Before submission, the process also confirms:
Identity documents
Address history
Right to work details (where applicable)
Errors here can delay the process significantly.
Why This is Important for Care Businesses
You get a complete safeguarding picture, not just a basic background check
You reduce the risk of hiring unsuitable staff
You stay compliant with CQC and safeguarding regulations
An enhanced DBS check is not just paperwork, it is a critical risk management tool for any caregiver business.
If you run a care business, you must follow the correct process to get an enhanced DBS CRB check for your staff. You cannot skip steps or apply informally, regulators expect a structured process.
Here is how to get an enhanced DBS CRB check:
Step 1: Employer or Umbrella Body Initiates the Check
You (the employer) must start the process.
If you process many checks yearly, you can register with DBS
If not, you must use an umbrella body
This is why many people searching “enhanced DBS check online” cannot complete it alone.
Step 2: Complete the Enhanced DBS Application Form
The applicant fills in the enhanced DBS application form (also called the enhanced DBS CRB form).
This includes:
Personal details
Full 5-year address history
Role information
Accuracy is critical; errors cause delays.
Step 3: Verify Identity Documents
You must verify the applicant’s identity before submission.
Required documents usually include:
Passport or driving licence
Proof of address
Supporting ID if needed
If details do not match, the application may be rejected.
Step 4: Submit the Application
You send the completed form to:
DBS (if registered), or
Your umbrella body
At this stage, the enhanced DBS check online process moves into review.
Step 5: DBS Processes the Check
The Disclosure and Barring Service:
Reviews criminal records
Contacts relevant police forces
Checks barred lists
This is the longest stage of the process.
Step 6: Certificate Issued to the Applicant
DBS sends the certificate directly to the applicant, not the employer.
You must ask the applicant to show it
You should verify authenticity before hiring
Key Tip for Care Providers
Always build this process into your recruitment workflow. Do not allow staff to start unsupervised work until you complete the enhanced DBS check.
A clear, compliant process protects your business and ensures you meet enhanced DBS CRB requirements.
Can You Apply for an Enhanced DBS Check for Yourself?
Disclosure and barring service (DBS)
Many people search “apply for enhanced DBS for myself” or “enhanced DBS check for myself”, but this often leads to confusion.
The truth is simple: You cannot apply for an enhanced DBS CRB check entirely by yourself.
Why You Cannot Apply Alone
The Disclosure and Barring Service only allows enhanced checks when:
A specific job role requires it
The role involves regulated activity
An employer or authorised organisation verifies the application
This ensures the check stays relevant to safeguarding, not general background screening.
How Individuals Actually Get an Enhanced DBS Check
If you need an enhanced DBS check, you must go through:
An employer (e.g. care agency, care home, NHS provider)
Or an umbrella body acting on behalf of the employer
The employer will:
Confirm the role qualifies for an enhanced check
Complete the application process
Verify your identity and documents
What If You Are Self-Employed?
If you work as a self-employed caregiver, you still cannot apply directly.
Instead, you must:
Work with an organisation that can request the check
Or use an umbrella body authorised to process enhanced DBS applications
Alternative Option (If You Just Need a Check)
If you only need a general background check (not for regulated care work), you can apply for a:
Basic DBS check
This shows unspent convictions only
You can apply for it yourself online
Key Takeaway for Care Businesses
If you hire caregivers, always remember:
The employer controls the enhanced DBS process
Individual applications without employer involvement are not valid
Understanding this prevents delays and ensures you meet enhanced DBS CRB requirements correctly.
One of the most common questions care providers ask is: how long does a DBS check take?
For an enhanced DBS CRB check, the process usually takes 7 to 14 days from submission to certificate issue.
Typical Timeline Breakdown
Application and ID verification: 1–3 days
DBS processing and police checks: 5–10 days
Certificate delivery: 1–3 days
Most applications fall within this range if everything is correct.
What Can Delay an Enhanced DBS Check?
Several factors can extend the timeline:
Incorrect or incomplete application details
Gaps in address history
Multiple police forces involved in checks
High application volumes
Even small errors can add several days to the process.
Can You Speed Up a DBS Check?
No, you cannot pay to fast-track the official DBS process.
However, you can reduce delays by:
Submitting accurate information
Verifying documents properly
Using experienced umbrella bodies
Why This Matters for Care Providers
Delays can slow down recruitment
You may need to supervise new staff temporarily
Poor planning can affect service delivery and compliance
Always start DBS checks early in your hiring process.
Pro Tip
Build DBS timelines into your recruitment planning so you never rely on last-minute checks. A proactive approach keeps your care service fully compliant and operational.
How Much Is an Enhanced DBS Check?
An enhanced DBS check costs £49.50, excluding any additional service fees charged by third-party providers. If you are hiring caregivers, you must understand how much a DBS check costs so you can budget correctly and avoid surprises.
Breakdown of Costs
Enhanced DBS check: £49.50
Enhanced DBS with barred lists: £49.50 (same base fee)
Volunteer checks: Free (in most cases)
The government sets these prices through the Disclosure and Barring Service.
Additional Service Fees
If you use an umbrella body or third-party provider, you may pay:
Processing or administration fees
Identity verification charges
Optional support services
These can increase the total cost beyond £49.50.
Who Pays for the DBS Check?
This depends on your organisation:
Some employers cover the full cost
Some share the cost with employees
Others require staff to pay upfront
In the care sector, many providers choose to cover the cost to attract and retain staff.
Why is This Important for Care Businesses?
DBS checks are a mandatory hiring expense
Costs can scale quickly if you recruit frequently
Budgeting properly helps maintain compliance without delays
Treat DBS checks as a core operational cost, not an optional extra.
Many care providers ask: how long does a DBS last? Or what is the enhanced DBS CRB validity? A DBS check has no official expiry date, but employers typically renew it every 1 to 3 years to maintain compliance.
Why There Is No Expiry Date
A DBS certificate reflects a person’s criminal record at the time it was issued.
It does not update automatically
New offences or changes will not appear on an old certificate
This is why relying on an outdated check can be risky.
How Often Should You Renew a DBS Check?
Although there is no legal expiry, most care providers:
Renew DBS checks every 1 to 3 years
Request a new check when:
A staff member changes role
There are safeguarding concerns
A contract requires updated compliance
Many commissioners and regulators expect recent DBS checks, not old ones.
Using the DBS Update Service
The update service allows you to:
Keep a DBS certificate up to date
Check an employee’s status online
Avoid repeated full applications
This is especially useful for care agencies with frequent recruitment.
Why This is Important for Care Businesses
Outdated checks can lead to compliance issues
You may fail inspections if records are not current
Regular updates protect both service users and your organisation
Treat DBS renewal as part of your ongoing safeguarding process.
DBS Tracking: How to Track Your Application
After submitting an application, many employers and applicants want to know how to track DBS progress. The good news is that you can monitor your application using the DBS tracking service. You can track DBS applications online using the Disclosure and Barring Service tracking service with your application reference number and date of birth.
How to Track a DBS Application
You can use the official Disclosure and Barring Service tracking service to check the status of an application.
To use the DBS tracking service, you will need:
Application reference number
Applicant’s date of birth
Once entered, the system shows the current stage of the check.
Stages You May See When You Track DBS
When using disclosure barring service tracking, your application may show:
Application received
ID verification completed
Police checks in progress
Certificate printed
Certificate dispatched
This helps you understand exactly where delays may occur.
Who Can Use DBS Tracking?
Employers (if they submitted the application)
Umbrella bodies managing the process
Applicants (with the correct reference details)
If you used an umbrella body, they may also provide their own tracking updates.
Why DBS Tracking Matters for Care Providers
Helps you plan staff onboarding timelines
Reduces uncertainty during recruitment
Allows you to follow up quickly if delays occur
This is especially important when hiring multiple caregivers at once.
The DBS Update Service is a subscription service that allows employers to check whether a DBS certificate remains up to date without submitting a new application each time.
What Is the DBS Update Service?
The update service lets you:
Check an employee’s DBS status online
Confirm if new information has been added since the certificate was issued
Avoid repeating full DBS applications
This makes it easier to manage compliance across your workforce.
How It Works
The employee registers for the update service after receiving their DBS certificate
The employer gets permission to check their status online
The system confirms whether the certificate is still valid or if changes exist
You do not see details, only whether the status has changed.
Cost of the Update Service
Annual subscription: £13 per year
Free for volunteers
This is a low-cost way to maintain continuous safeguarding checks.
For Care Businesses, This:
Reduces the need for repeated DBS applications
Speeds up recruitment and onboarding
Helps maintain ongoing compliance with safeguarding standards
For agencies hiring frequently, this can save both time and money.
When You Should Still Request a New DBS Check
Even with the update service, you should request a new check if:
The employee changes role significantly
The check level is no longer appropriate
You cannot verify continuous subscription
Basic vs Enhanced DBS: What’s the Difference?
A basic DBS check shows only unspent convictions, while an enhanced DBS check includes full criminal history, police intelligence, and barred list checks required for roles involving vulnerable people.
Care providers often compare a basic DBS check with an enhanced DBS CRB check, but the difference is significant. Choosing the wrong level can lead to compliance issues.
Key Differences at a Glance
Feature
Basic DBS Check
Enhanced DBS CRB Check
Criminal records
Unspent convictions only
Spent + unspent convictions, cautions
Police intelligence
Not included
Included (if relevant)
Barred lists
Not included
Included (if required)
Who can apply
Individuals or employers
Employers or umbrella bodies only
Typical use
General employment checks
Care, healthcare, education roles
When to Use a Basic DBS Check
A basic DBS check is suitable when:
The role does not involve vulnerable people
You need a general background check
The position is low-risk from a safeguarding perspective
Individuals can apply for this check themselves.
When to Use an Enhanced DBS Check
An enhanced CRB DBS check is required when:
The role involves regulated activity
Staff provide personal care or healthcare support
There is direct contact with vulnerable adults or children
This is the standard requirement in the care sector.
Importance for Care Providers
Using the wrong check can lead to regulatory breaches
You may fail inspections if safeguarding checks are inadequate
Commissioners often require enhanced DBS checks as standard
Always match the check level to the role.
Common DBS Mistakes Care Providers Must Avoid
Even experienced care providers make mistakes when handling enhanced DBS CRB checks. These errors can delay recruitment, fail inspections, or expose your business to safeguarding risks.
1. Allowing Staff to Start Without a DBS Check
Some providers let staff begin work before completing checks.
This is risky.
Staff must not carry out unsupervised regulated activity without a valid DBS check
Regulators may flag this during inspections
2. Using Outdated DBS Certificates
Many employers assume a DBS check lasts forever.
It does not update automatically.
Old certificates may not reflect new offences
This can create serious safeguarding gaps
3. Requesting the Wrong Level of Check
Using a basic DBS check for a caregiver role is a common mistake.
In care settings, you usually need an enhanced CRB DBS check.
4. Poor Identity Verification
Errors in ID checks can:
Delay applications
Lead to rejection
Cause compliance issues
Always verify documents carefully before submission.
5. Not Checking Barred List Requirements
Some employers forget to request barred list checks when needed.
This is a critical safeguarding failure.
You must check barred lists for regulated roles
Failing to do so can have legal consequences
6. Ignoring DBS Tracking
Not using the dbs tracking service can leave you in the dark.
You should always:
Track application progress
Follow up on delays early
7. Not Using the Update Service
Skipping the update service leads to:
Repeated applications
Higher costs
Slower hiring
Many providers overlook this simple efficiency tool.
Mistakes can lead to failed CQC inspections
You risk hiring unsuitable staff
Your reputation and contracts may suffer
Strong DBS processes protect both your clients and your business.
Quick Tip
Build a standard DBS workflow into your recruitment process, so every check is consistent, compliant, and easy to track.
Final Thoughts…
An enhanced DBS CRB check ensures that caregivers and healthcare staff are safe to work with vulnerable people by providing a full background check, including criminal records, police intelligence, and barred list status.
It is more than a recruitment step; it is a core part of running a safe, compliant, and trusted care service.
If you manage a care business, every hiring decision directly affects:
The safety of vulnerable people
Your regulatory compliance
Your reputation with families and commissioners
What Smart Care Providers Do Differently
Successful care providers:
Start DBS checks early in the hiring process
Use structured workflows for every application
Keep records up to date and verifiable
Use tools like DBS tracking and the update service
Never compromise on safeguarding standards
They treat DBS checks as a business-critical system, not admin.
The Bigger Picture
Strong DBS processes help you:
Pass inspections with confidence
Win and retain government contracts
Build trust with service users and families
Reduce risk across your organisation
In today’s care sector, compliance is not optional; it is your competitive advantage.
Need Help with DBS Compliance or Care Business Setup?
At Care Sync Experts, we help care providers stay compliant, win contracts, and grow with confidence.
Whether you need support with:
Enhanced DBS processes and safeguarding compliance
CQC registration and inspection readiness
Tender writing and contract acquisition
Policies, documentation, and operational setup
We’ve got you covered.
Don’t risk delays, failed inspections, or lost opportunities.
Let our experts handle the complexity so you can focus on delivering quality care.
Book a consultation with Care Sync Experts and take the next step toward building a compliant, scalable care business.
FAQ
What does DBS stand for?
DBS stands for the Disclosure and Barring Service. It is the UK government body responsible for carrying out background checks to help employers make safer recruitment decisions, especially in sectors like healthcare, education, and social care.
What does a DBS check show?
A DBS check shows an individual’s criminal record history, depending on the level of the check. Basic DBS check: Unspent convictions only Enhanced DBS CRB check: Spent and unspent convictions, cautions, police intelligence, and barred list status (if requested)
Employers use this information to assess whether someone is suitable to work with vulnerable people.
What is a CRB check?
A CRB check is the old name for what is now called a DBS check. CRB stood for Criminal Records Bureau It was replaced by the Disclosure and Barring Service (DBS) in 2012 Today, people still use the term “CRB check,” but it means the same as a DBS check.
How long does an enhanced DBS check take?
An enhanced DBS check typically takes 7 to 14 days to complete. However, it may take longer if: – Multiple police forces need to review the application – The information provided is incorrect or incomplete – Most delays happen due to errors or additional checks, so accuracy is key when applying.
A central reservations system in caregiving is a digital platform that allows care providers to manage bookings, staff scheduling, and care delivery from a single system.
In the UK, these systems help domiciliary care agencies and care homes coordinate visits, maintain accurate care records, and meet compliance standards efficiently.
In simple terms, what is a central reservation system? It is a tool that replaces manual booking, rota planning, and paper-based care logs with a centralised, real-time system designed to improve care delivery and operational control.
Key Takeaways
A central reservations system helps care providers manage bookings, staff rotas, and care plans in one place
UK care businesses use these systems to improve efficiency and meet CQC compliance requirements
Digital systems replace paper logs with real-time, secure care records
Platforms often include features like scheduling, visit tracking, and mobile access for carers
Tools such as Log my care, CarePlanner login, and Birdi software support digital care management
Centralised systems reduce admin workload and improve visibility across care operations
A central reservations system in care is a digital system that manages bookings, staff scheduling, and care delivery from one central platform. It allows care providers to organise visits, assign carers, and track services in real time without relying on paper or disconnected tools.
So, what is central reservation in the care context?
It is the process of coordinating all care-related bookings, such as home visits, shift allocations, and service delivery, through a single, centralised system.
In broader terms, the central reservation meaning comes from industries like hotels and travel, where a central reservation system manages room bookings across multiple locations. In care, the concept works differently. Instead of rooms, providers manage:
client visits
staff rotas
care delivery schedules
This often raises questions like:
what’s a central reservation system in care?
what’s central reservation compared to traditional scheduling?
The answer is simple: it replaces manual coordination with a structured, digital workflow.
For example, instead of:
answering calls to book visits
updating paper rota sheets
manually checking care plans
a central reservations system allows teams to:
book visits instantly
assign carers based on availability
access care plans and updates in real time
This shift gives care providers better control over daily operations while reducing errors and missed appointments.
At its core, a central reservations system is not just about booking, it is about connecting every part of care delivery into one reliable system.
How Central Reservation Systems Work in Caregiver Operations
A central reservations system brings together booking, scheduling, and care delivery into one smooth workflow. Instead of juggling calls, paper logs, and separate tools, care providers manage everything from a single platform.
Here’s how it works in real caregiver operations:
1. Booking and Visit Allocation
Staff or coordinators enter new care requests into the system. This could be:
a new client needing daily visits
a family booking a care slot
an urgent same-day request
The system logs the booking instantly and makes it visible to the entire team. This replaces manual processes like phone bookings and handwritten logs.
2. Staff Scheduling and Rotas
Once a visit is booked, the system assigns carers based on:
availability
location
skills and qualifications
Instead of updating spreadsheets or rota sheets, managers adjust schedules in real time.
This ensures no missed visits and better workload balance.
3. Care Plan Access and Updates
Carers access client information directly from the system, including:
care plan template details
medication instructions
visit notes and history
They no longer need printed documents or separate files. Everything stays updated in one place.
4. Real-Time Logging and Communication
During or after visits, carers log activities using mobile apps or portals (often referred to as log in care systems). They can:
record completed tasks
update notes
flag issues instantly
Managers see updates in real time, which improves oversight and response speed.
5. Monitoring and Compliance Tracking
The system automatically tracks:
visit times and attendance
completed care tasks
audit trails for inspections
This makes it easier to prepare for CQC inspections and maintain compliance without scrambling for records.
Without a central reservation workflow, teams rely on:
phone calls
paper records
disconnected tools
With a central reservations system, everything connects:
bookings → schedules → care delivery → reporting
The result is fewer errors, faster coordination, and more time focused on actual care instead of admin.
Why UK Care Providers Are Moving to Central Reservation Systems
Central Reservation
Care providers across the UK are moving to a central reservations system because manual processes no longer keep up with the demands of modern care delivery.
Most teams recognise the same daily challenges:
constant phone calls to book or change visits
rota clashes and last-minute gaps
missing or incomplete care records
pressure to stay compliant with CQC standards
A central reservation approach removes these problems by giving providers full control over their operations.
1. Reducing Admin Pressure on Staff
Reception and care coordinators often spend hours managing bookings manually. Each call interrupts workflow and increases the risk of errors.
With a central reservations system, teams:
book visits in seconds
update schedules instantly
reduce back-and-forth communication
Staff spend less time on admin and more time supporting care delivery.
2. Improving Compliance and Inspection Readiness
UK regulators expect accurate, accessible records at all times. Paper logs and scattered systems make this difficult.
A digital system:
stores all visit and care data securely
creates automatic audit trails
allows instant access during inspections
This makes CQC inspections far less stressful and more predictable.
3. Enhancing Visibility Across the Organisation
Managers need to know what is happening in real time:
who is on shift
which visits are completed
where issues are occurring
A central reservations system provides a live overview of operations, helping teams respond quickly and make better decisions.
4. Improving the Experience for Families and Clients
Families expect convenience and transparency. Manual booking systems often lead to:
missed appointments
unclear schedules
delays in communication
With digital booking and scheduling:
visits are confirmed instantly
updates are communicated clearly
service delivery becomes more reliable
This builds trust and improves satisfaction.
5. Supporting Growth Without Losing Control
As care businesses grow, manual systems break down quickly. More clients and staff mean more complexity.
Key Features to Look For in a Central Reservations System
Not all platforms offer the same value. A good central reservations system should support the full care workflow, from booking visits to managing compliance, without adding complexity.
Here are the key features UK care providers should prioritise:
1. Digital Booking and Scheduling
The system should allow teams to:
book visits quickly
adjust schedules in real time
avoid double bookings or missed appointments
A strong booking engine replaces manual coordination and keeps operations organised.
2. Staff Rota and Workforce Management
Look for tools that manage:
staff availability
shift allocation
travel time between visits
Platforms like The Care Office and CarePlanner login systems already offer structured rota management, helping coordinators balance workloads efficiently.
3. Mobile Access for Carers
Carers need access on the go. A modern system should allow them to:
log visits in real time (log in care)
update notes instantly
confirm completed tasks
Solutions such as Log my care and Birdi software provide mobile-friendly access, making it easier for carers to stay connected while working in the community.
4. Digital Care Plans and Records
A reliable system should include:
structured care plan template access
medication records
daily care notes
This ensures carers always work with up-to-date information and reduces reliance on paper files.
5. Real-Time Monitoring and Alerts
Managers should be able to track:
missed or late visits
staff attendance
urgent care updates
Real-time alerts help teams act quickly and maintain service quality.
6. Compliance and Audit Trails
Compliance is non-negotiable in UK care.
The system must:
store secure, time-stamped records
provide full audit trails
support CQC inspection requirements
This removes the need to manually compile records during inspections.
7. Reporting and Insights
A strong central reservation platform should generate reports on:
service delivery
staff performance
client care trends
These insights help providers improve operations and make informed decisions.
What This Means in Practice
When these features work together, a central reservations system becomes more than just a booking tool.
It becomes a complete operational system that connects:
bookings
staff
care delivery
compliance
The right system does not just organise your care service, it helps you run it better, with fewer errors and more confidence.
A central reservations system for caregivers UK NHS context is not a single national booking platform, but a group of digital systems that support care coordination, record-keeping, and service delivery across health and social care.
In practice, care providers use centralised systems to align with NHS expectations around:
digital care records
data sharing
coordinated care delivery
How Central Systems Connect with NHS Workflows
Many UK care providers work alongside:
Primary Care Networks (PCNs)
GP services
NHS-funded care packages
A central reservations system supports this by:
organising care visits efficiently
keeping accurate, up-to-date records
making information easier to share when required
This improves communication between care providers and healthcare professionals.
Digital Social Care Records (DSCR)
The NHS has encouraged the adoption of Digital Social Care Records, which align closely with central reservation systems.
These records allow providers to:
store care data securely
access client information in real time
reduce paperwork across services
A central reservations system often acts as the foundation for these digital records.
Data Protection and GDPR Compliance
Handling care data requires strict compliance with UK regulations.
A good system must:
protect sensitive client information
control user access levels
maintain secure audit trails
This ensures providers meet both GDPR and NHS data handling expectations.
Using a central reservations system aligned with NHS standards helps providers:
deliver more coordinated care
reduce duplication of work
improve communication across services
stay compliant with national digital care initiatives
Cost of a Central Reservations System for Caregivers in the UK
The cost of a central reservations system for caregivers UK varies depending on the size of the organisation, the features required, and the number of users.
Most UK care providers can expect to pay between:
£150 to £300 per month for small to mid-sized agencies
£300 to £500+ per month for larger providers with advanced features
Additional setup or training fees (in some cases)
What Affects the Cost?
Several factors influence pricing:
1. Number of Clients and Staff
Systems often scale based on:
number of service users
number of carers using the platform
Larger teams typically pay more.
2. Features and Functionality
Basic systems include:
scheduling
visit logging
simple reporting
Advanced platforms add:
real-time alerts
integrations with other systems
detailed analytics and compliance tools
More features = higher cost.
3. Level of Support and Training
Some providers include:
onboarding support
staff training
ongoing customer service
Premium support may increase monthly fees but improves adoption.
Is It Worth the Cost?
For most care providers, the return on investment is clear.
A central reservations system helps reduce:
admin hours spent on booking and scheduling
missed visits and costly errors
compliance risks during inspections
For example:
saving 10–15 staff hours per week can easily offset the monthly fee
avoiding one compliance issue can save thousands in potential penalties
Should Your Care Business Use a Central Reservation System?
How Does a Central Reservation System (CRS) Work
Not every care provider adopts a central reservations system at the same stage, but most reach a point where manual processes stop working.
Here’s how to decide if it’s the right move for your organisation.
You Should Use a Central Reservations System If:
1. You Struggle with Scheduling and Missed Visits
If your team relies on:
phone calls
spreadsheets
paper rotas
you are likely dealing with:
double bookings
missed visits
last-minute confusion
A central reservation system removes these issues by organising everything in one place.
2. Admin Work Is Taking Too Much Time
If your staff spend hours:
answering booking calls
updating schedules
chasing information
A digital system can automate most of these tasks and free up time for care.
3. You Need Better Compliance and Record-Keeping
If preparing for inspections feels stressful or rushed, your current system may not be reliable.
A central reservations system helps by:
storing accurate, time-stamped records
providing instant access to data
reducing compliance risks
4. Your Service Is Growing
As your business expands:
more clients
more staff
more visits
Manual systems become harder to manage.
A central reservation approach allows you to scale without losing control.
You May Not Need One Yet If:
You manage a very small number of clients
Your operations are simple and stable
You can track everything accurately without delays
Even then, growth will eventually create pressure to switch.
The Real Question to Ask
Instead of asking: “Do we need a central reservations system?”
Ask: “How much time and risk are we carrying by not using one?”
Conclusion
A central reservations system is quickly becoming a core part of how modern care services operate in the UK. It brings booking, scheduling, and care delivery into one structured system, giving providers better control over their day-to-day operations.
For caregivers, the impact is immediate:
less time spent on admin
fewer missed visits
clearer communication across teams
stronger compliance with regulatory standards
For managers and business owners, it creates something even more valuable: visibility and confidence. You can see what is happening across your service in real time, respond quickly to issues, and scale without losing control.
The shift from manual processes to a central reservation approach is not just about technology. It is about running a safer, more reliable, and more efficient care service.
What This Means for Your Care Business
If you are still relying on paper logs, phone bookings, or disconnected tools, you are likely:
losing valuable staff time
increasing the risk of errors
making compliance harder than it needs to be
A central reservations system for caregivers UK gives you a clear path forward, one where operations are organised, records are accurate, and your team can focus on what matters most: delivering quality care.
Care providers who adopt centralised systems early gain a strong operational advantage. They run smoother services, handle growth better, and build more trust with families and regulators.
If you want to stay competitive and in control, now is the time to move towards a central reservations system that supports your care business today and scales with you tomorrow.
Need Expert Support Choosing and Implementing the Right Care Management System?
Care Sync Experts supports care providers, domiciliary care agencies, and care home operators across the UK with clear, practical guidance on selecting and implementing the right central reservations system for their services.
From helping you understand how digital care systems work to advising on platforms like Log my care, CarePlanner, Birdi software, and other care management tools, our specialists break down complex technology into simple, actionable decisions.
Whether you are moving away from paper-based systems, improving scheduling and compliance, or scaling your operations with a centralised digital solution, our team provides tailored support designed for real-world care environments.
Choose the right system, avoid costly implementation mistakes, and ensure your care service runs efficiently, remains compliant, and delivers high-quality care.
Contact Care Sync Experts today to get expert guidance on care management systems, central reservations solutions, and building a smarter, more connected care operation.
FAQ
Who are the largest care home providers in the UK?
The largest care home providers in the UK include organisations such as HC-One, Barchester Healthcare, Four Seasons Health Care, Care UK, and Anchor.
These providers operate across multiple locations and manage thousands of residents, often using advanced digital systems to handle staffing, care planning, and compliance at scale.
What is the care system in the UK?
The care system in the UK combines publicly funded and privately delivered services to support individuals who need help with daily living.
Local authorities and the NHS fund or arrange care based on eligibility, while independent providers, such as care homes and domiciliary care agencies – deliver most services.
Regulators like the CQC (England), CIW (Wales), and RQIA (Northern Ireland) oversee quality and safety.
Who funds care homes in the UK?
Care homes in the UK are funded through a mix of: – Local authority funding (for eligible individuals) – NHS funding (for specific healthcare needs, such as Continuing Healthcare) – Private payments (self-funded residents)
In many cases, funding is shared, depending on the individual’s financial situation and care requirements.
What are the top 3 qualities of a caregiver?
The three most important qualities of a caregiver are: Compassion: The ability to provide emotional support and treat individuals with dignity and respect Reliability: Being consistent, punctual, and dependable in delivering care Communication skills: Clearly understanding and responding to the needs of clients, families, and healthcare professionals
These qualities directly impact the quality of care and overall client experience.
Part L building regulations are UK rules that set minimum energy efficiency standards for buildings, including how they are designed, heated, insulated, and ventilated. In England, these requirements are explained in Approved Document L, which applies to both new buildings and existing properties undergoing renovation or extension.
For care businesses, Part L UK matters whenever you build, convert, extend, or upgrade a property. Whether you are opening a new care home, converting a house into supported living, or improving an office space, you must meet Part L compliance standards before the building can be approved for use.
The latest updates, often referred to as Part L building regulations 2022, came into effect on 15 June 2022 under the Part L building regulations 2021 framework (with later amendments). These changes introduced stricter requirements to reduce energy use and carbon emissions, as part of the UK’s wider push toward net zero.
In simple terms, building regs Part L ensure that:
Buildings lose less heat through walls, roofs, and windows
Heating systems run efficiently and use less energy
Ventilation systems maintain air quality without wasting heat
Developers and contractors provide clear evidence that work meets required standards
For care providers, this is not just a technical requirement. It directly affects:
resident comfort and safety
energy costs and long-term operating expenses
whether a building can legally open or continue operating
Understanding Part L building regulations early helps care businesses avoid delays, reduce costs, and make smarter decisions when planning or upgrading their services.
Care businesses cannot treat Part L building regulations as a “builder’s problem.” These rules directly affect how you open, run, and scale your service.
Energy efficiency is not just about compliance; it shapes your daily operations.
1. It directly impacts your running costs
Care homes and supported living services operate 24/7. Heating, hot water, and ventilation run constantly.
Poor Part L compliance means:
higher energy bills
inefficient heating systems
long-term financial pressure
Meeting building regs Part L standards helps you reduce energy waste and protect your margins.
2. It affects resident comfort and care quality
Warm, well-ventilated environments are essential in care settings.
Strong insulation and proper Part L building Regulations ventilation improve:
indoor temperature stability
air quality for vulnerable residents
infection control and overall wellbeing
If you get this wrong, you don’t just fail compliance, you compromise care standards.
3. It determines whether your project can open on time
If your building fails Part L UK requirements, building control can delay or block approval.
This can lead to:
delayed service launch
lost revenue
costly redesigns or rework
Many care providers only discover issues late, when fixes become expensive and disruptive.
4. It influences funding, inspections, and reputation
Part L building regulations focus on how a building uses energy and how much heat it loses. In England, Approved Document L explains how to meet these requirements in practice.
For care businesses, this section answers a simple question: What exactly do we need to get right before a building is approved?
1. Two main categories: dwellings vs non-dwellings
Part L UK splits buildings into two groups:
Dwellings (Part L1A / L1B)
Homes where people live independently (e.g. some supported living setups)
Non-dwellings (Part L2A / L2B)
Commercial or institutional spaces (e.g. care homes, offices, clinics)
Most care homes fall under Part L building regulations non dwellings, while supported living can fall under either category depending on layout and level of independence.
Getting this classification wrong can lead to incorrect design, failed approval, and delays.
2. Fabric performance (how well the building retains heat)
Building regs Part L require strong insulation across:
walls
roofs
floors
windows and doors
This is measured using U-values (how much heat escapes).
For care providers, this means:
better temperature control for residents
reduced heating demand
lower long-term costs
3. Heating and hot water systems
Part L building regulations push for more efficient, low-carbon systems.
This includes:
modern boilers or heat pumps
lower flow temperatures
smarter controls
For care environments, heating must balance:
energy efficiency
consistent warmth for vulnerable residents
4. Ventilation and air quality
Part L building Regulations ventilation works alongside other rules to ensure buildings stay healthy as they become more airtight.
This includes:
mechanical or natural ventilation systems
controlled airflow
reduced heat loss while maintaining fresh air
This is critical in care settings, where air quality directly affects health outcomes.
5. Energy modelling and calculations
To prove compliance, developers must use:
SAP (for dwellings)
SBEM (for non-dwellings)
These models calculate:
energy use
carbon emissions
overall efficiency
Care businesses don’t need to run these models, but you must ensure your project team does.
6. Evidence and documentation
One of the biggest changes under Part L building regulations 2022 is stricter proof requirements.
You must provide:
design-stage calculations
as-built performance reports
photographic evidence of construction details
Without this, you cannot demonstrate Part L compliance, even if the building is physically correct.
Approved Document L is not just guidance, it defines what your building must achieve to pass.
For care providers, it covers:
how your building is built
how it performs
how you prove it meets the rules
Understanding this early helps you avoid costly mistakes and ensures your project meets Part L building regulations from day one.
Many care providers assume Part L building regulations only apply to large construction projects. In reality, they affect almost every type of property change in the care sector.
If you run or plan to expand a care business, you will likely trigger Part L compliance at some point.
1. Opening a new care home
New-build care homes fall fully under building regs Part L, usually within the Part L building regulations non dwellings category.
You must meet strict requirements for:
insulation and airtightness
heating system efficiency
ventilation design
full energy modelling and evidence
These projects must align with Part L building regulations 2022, which introduced tighter carbon reduction targets.
2. Converting buildings into supported living
Conversions are common in the care sector, but they come with risk.
If you convert:
a house into supported living
a commercial building into a care facility
You must meet Part L building regulations 2021 standards for existing buildings.
This often means:
upgrading insulation
improving heating systems
meeting minimum energy performance levels
Many providers underestimate how much upgrade work is required.
3. Extending an existing care home
Adding new rooms, wings, or facilities triggers Part L UK requirements.
You must ensure:
the new extension meets current energy standards
the connection between old and new parts does not create heat loss issues
Even small extensions can require significant upgrades to meet compliance.
4. Refurbishing or upgrading existing buildings
Even if you are not building new, Part L building regulations still apply when you:
replace windows or doors
upgrade insulation
install a new heating system
carry out major renovation work
These fall under Part L1B or L2B, depending on the building type.
Many care providers trigger compliance without realising it.
5. Setting up or upgrading a domiciliary care office
Office spaces may seem simple, but they still fall under building regs Part L.
If you:
move into a new office
refit an existing one
upgrade heating or ventilation
You may need to meet energy efficiency standards and provide compliance evidence.
6. Special cases and older buildings
Some care providers operate in older or unique properties, such as a grade 2 listed building.
In these cases:
full compliance may not always be possible
adjustments or alternative approaches may apply
However, you should never assume exemption without expert advice under Part L building Regulations exemptions.
Part L Requirements Care Providers Should Understand Before Starting Work
Before you start any project, you need a clear understanding of what Part L building regulations actually require in practice. This is where many care businesses make costly mistakes, by relying entirely on contractors without understanding the basics.
1. Insulation and building fabric
Building regs Part L place strong emphasis on how well your building retains heat.
You must ensure:
walls, roofs, and floors meet minimum insulation standards
windows and doors limit heat loss
gaps and air leakage are controlled
Better insulation means:
more stable indoor temperatures
improved comfort for residents
lower energy bills over time
2. Heating and hot water systems
Part L building regulations 2022 push for more efficient and lower-carbon systems.
Your project must include:
energy-efficient boilers or heat pumps
properly sized systems for the building
modern controls to manage temperature effectively
In care settings, you must balance efficiency with reliability, residents cannot tolerate inconsistent heating.
3. Ventilation and air quality
As buildings become more airtight, ventilation becomes critical.
Part L building Regulations ventilation ensures:
fresh air circulation
removal of moisture and pollutants
reduced risk of overheating
This often includes:
mechanical ventilation systems
heat recovery systems in some cases
Poor ventilation can lead to:
damp and mould
poor air quality
increased health risks for residents
4. Energy modelling and performance targets
To prove Part L compliance, your project team must complete energy calculations.
These include:
SAP for dwellings
SBEM for non-dwellings
These models assess:
carbon emissions
energy consumption
overall building performance
You don’t need to run these models yourself, but you must ensure they are completed correctly.
5. Evidence and documentation (often overlooked)
One of the biggest shifts in Part L UK is the requirement to prove compliance, not just claim it.
You must provide:
design-stage energy reports
as-built performance reports
photographic evidence of key construction stages
Photos must clearly show:
insulation installation
junction details where heat loss can occur
key building elements before they are covered
Without proper evidence, your building may fail approval, even if the work is correct.
6. Responsibility and coordination
Many care providers assume the builder handles everything.
How Part L Links with Other Rules Care Businesses May Hear About
Part L Building Regulations Compliance
When you plan a care project, you will hear multiple regulations, not just Part L building regulations. This can feel overwhelming, especially if you are not from a construction background.
The key is to understand what each rule covers and how they connect.
1. Part L vs the Building Safety Act
Part L focuses on energy efficiency. The Building Safety Act and building safety act 2022 focus on safety, accountability, and documentation.
For care providers, this means:
Part L ensures your building performs efficiently
The Building Safety Act ensures your building is safe and properly documented
Both require strong record-keeping and evidence, especially for larger or higher-risk buildings.
2. Part L vs Part M (accessibility)
You will often hear about part m building regulations or approved document m during care projects.
Part L = energy efficiency
Part M = accessibility and usability
In care settings, building regs part m is critical because it covers:
wheelchair access
bathroom layouts
safe movement within the building
You must meet both standards at the same time; one does not replace the other.
3. Part L vs fire safety rules (Part B)
Fire safety falls under:
approved doc b
building regs part b
These rules focus on:
fire detection systems
escape routes
compartmentation
While Part L UK focuses on insulation and airtightness, you must ensure these do not conflict with fire safety design.
4. Other related regulations you may encounter
Depending on your project, you may also hear about:
approved document k (safety around stairs, ramps, and movement)
general building regulations covering structure and ventilation
These do not replace Part L building regulations, but they run alongside them.
5. Why this matters for care providers
Care projects rarely deal with one regulation in isolation.
If you:
build a new care home
convert a property
extend an existing facility
You will need to meet multiple standards at once.
The biggest risk is:
focusing on energy efficiency
while overlooking access, safety, or usability
Part L building regulations form just one part of a wider compliance framework.
For care providers:
Part L = energy performance
Part M = accessibility
Part B = fire safety
Building Safety Act = accountability and safety systems
Understanding how they work together helps you:
avoid design conflicts
prevent costly redesigns
ensure your building meets all approval requirements the first time
Are there any exemptions or special cases under Part L?
Changing Part L Thermal Standards
Many care providers ask whether Part L building regulations always apply in full. The answer is: not always, but exemptions are limited and highly controlled.
You should never assume you qualify for Part L building Regulations exemptions without proper advice.
1. Existing and older buildings
When you upgrade an existing property, Part L allows some flexibility.
For example:
you may not need to upgrade every element to new-build standards
improvements must be “reasonable and practical”
However, you still need to:
improve energy performance where possible
avoid making the building worse
Even partial refurbishment can still trigger Part L compliance requirements.
2. Listed and heritage buildings
Care providers sometimes operate in older or historic properties, such as a grade 2 listed building.
In these cases:
strict upgrades (like replacing windows or external insulation) may not be allowed
heritage protection can limit what changes you can make
However:
you must still improve energy efficiency where it does not damage the building’s character
This often requires:
specialist advice
tailored solutions
3. Technical and practical limitations
Some buildings cannot meet full modern standards due to:
structural limitations
space constraints
compatibility with existing systems
In these situations:
alternative measures may be accepted
compliance focuses on “reasonable improvement” rather than perfection
4. What does NOT count as an exemption
Care providers often misunderstand this.
You are not exempt just because:
the building is old
the project is small
you are only making minor changes
you are leasing the property
If your work affects energy performance, building regs Part L will likely apply.
5. Why exemptions still require documentation
Even when flexibility applies, you must:
justify your approach
document decisions
show why full compliance was not possible
Building control will still expect:
clear reasoning
supporting evidence
Part L building regulations rarely offer full exemptions.
In most cases:
you must comply fully
or improve performance as far as reasonably possible
Care providers who assume they are exempt often face:
delays
redesign costs
compliance issues during approval
The safest approach is simple:
Always check early, plan properly, and treat Part L compliance as part of your core project strategy.
Many care providers run into problems with Part L building regulations, not because the rules are unclear, but because they get involved too late or rely on the wrong assumptions.
Avoiding these mistakes can save you time, money, and project delays.
1. Treating Part L as the builder’s responsibility
Many providers assume the contractor will “handle compliance.”
In reality:
you own the project
you remain responsible for Part L compliance
poor coordination can still lead to failure
You need visibility from design to completion.
2. Signing a lease or buying a property without checking requirements
This is one of the most expensive mistakes.
Care providers often:
secure a building first
check building regs Part L later
This can lead to:
unexpected upgrade costs
delays in opening
redesign of heating, insulation, or ventilation systems
Always assess Part L building regulations before committing to a property.
3. Assuming only new builds are affected
Many providers think Part L UK only applies to new construction.
In reality, it also applies when you:
refurbish
extend
replace key building elements
Even simple upgrades can trigger compliance requirements.
4. Ignoring ventilation when improving insulation
Improving insulation without considering Part L building Regulations ventilation creates serious problems.
This can lead to:
poor air quality
damp and mould
overheating
Energy efficiency must always balance with ventilation.
5. Underestimating documentation and evidence
Some providers focus on the physical build but forget about proof.
Under Part L building regulations 2022, you must provide:
energy calculations
as-built reports
photographic evidence
Without this, your project may fail, even if everything is installed correctly.
6. Leaving compliance too late in the project
If you only think about Part L during construction, you are already at risk.
Late changes can mean:
redesigning systems
replacing materials
increased costs
The best projects consider compliance at the design stage.
7. Not involving the right professionals early
Successful projects require:
energy assessors
consultants
experienced contractors
If you delay bringing them in:
mistakes go unnoticed
compliance gaps increase
Bottom line
Most Part L building regulations issues come down to timing and awareness.
Care providers who:
plan early
ask the right questions
stay involved
Avoid delays, reduce costs, and achieve smooth approvals.
Those who don’t often face:
rework
compliance failures
delayed service launches
Final takeaway for care providers
Part L building regulations are not just a technical requirement, they directly shape how your care business operates, grows, and delivers safe environments.
If you plan to:
open a new service
convert a property
extend or refurbish a building
You must consider Part L compliance from the very beginning.
Care providers who approach Part L UK correctly:
control energy costs
create comfortable, healthy environments for residents
avoid delays during approval
protect their investment
Those who ignore it often face:
unexpected upgrade costs
failed inspections
delayed openings
The simple rule to follow
Treat building regs Part L as a business priority, not just a construction detail.
If you:
check requirements early
work with the right professionals
plan for both performance and evidence
You will meet compliance smoothly and avoid costly mistakes.
One final perspective
Energy efficiency is no longer optional. It sits at the centre of modern care delivery.
Understanding Part L building regulations helps you:
build smarter
operate more efficiently
deliver better care environments
And in a sector where comfort, safety, and sustainability matter every day…
That is a competitive advantage.
Need Expert Support Navigating Building Compliance and Care Facility Requirements?
Care Sync Experts supports care providers, care home operators, and healthcare organisations across the UK with clear, practical guidance on regulatory compliance, property requirements, and operational readiness.
From helping you understand Part L building regulations, energy efficiency standards, and building compliance requirements, to guiding you through property conversions, refurbishments, and service setup, our specialists turn complex regulations into simple, actionable steps.
Whether you are opening a new care home, converting a property into supported living, upgrading your facilities, or ensuring full Part L compliance alongside CQC expectations, our team delivers tailored support designed for real-world care environments.
Plan smarter, avoid costly mistakes, and ensure your care premises meet all regulatory standards from day one.
Contact Care Sync Experts today to get expert support on building compliance, care facility setup, and navigating UK care regulations with confidence.
FAQ
Is Part L law in the UK?
Yes. Part L building regulations form part of the Building Regulations in England and are legally enforceable. While Approved Document L provides guidance on how to meet the requirements, the underlying regulation itself is law.
If a care provider or developer fails to meet Part L compliance, building control can: – refuse approval – require corrective work – issue fines or enforcement action In simple terms: you must comply with Part L to legally complete and use a building.
What are carbon emission targets in Part L?
Part L building regulations 2022 introduced stricter carbon reduction targets as part of the UK’s journey toward net zero.
For new buildings: – new homes must reduce carbon emissions by around 30% compared to previous standards – future standards aim for 75–80% reductions by 2025
For care providers, this means: – more efficient heating systems – better insulation – lower overall energy use
These targets directly influence design, costs, and long-term energy performance.
What is the 10 year rule for listed buildings?
The “10-year rule” is often misunderstood. It does not automatically exempt buildings from regulation, including Part L building regulations.
In planning terms, it generally refers to situations where: – unauthorised work may become lawful after 10 years if no enforcement action is taken
However, for buildings such as a grade 2 listed building: – separate listed building consent rules still apply – energy upgrades must balance compliance with heritage protection
Care providers should always seek professional advice; never assume older or listed buildings are exempt from compliance requirements.
What are the 7 stages of construction?
Understanding the construction process helps care providers manage Part L compliance effectively. The typical stages are: – Planning and feasibility – Design and approvals – Procurement and contractor selection – Site preparation – Construction – Inspection and compliance checks – Completion and handover
Part L building regulations apply across multiple stages, especially: – design (energy modelling and specifications) – construction (installation quality) – completion (evidence and certification)
Getting involved early in these stages helps care businesses avoid delays and ensure smooth approval.
The care certificate is a set of 16 standards that define the knowledge, skills, and behaviours every new health and social care worker must demonstrate to deliver safe, compassionate, and person-centred care.
Employers use it as part of induction for roles such as caregivers, support workers, and healthcare assistants. The Care Certificate standards (updated in 2025) ensure you understand essential areas like safeguarding, communication, and duty of care within real care settings.
Key Takeaways
The care certificate includes 16 Care Certificate standards that every new care worker must complete.
You can start training through a care certificate online course, but your employer must assess you in the workplace.
The certificate prepares you for real roles in health and social care, including domiciliary care and care homes.
It covers key topics like safeguarding, communication, and the duty of care meaning in everyday practice.
Most employers expect you to complete it during your induction, especially if you are new to social care.
The certificate does not expire, but you must keep your knowledge updated as standards advance.
If you’re starting a role in care, the care certificate gives you the foundation you need to work safely and confidently from day one.
In simple terms, the care certificate teaches you how to care for people properly. It focuses on real situations you will face every day, supporting vulnerable adults, communicating clearly, protecting people from harm, and delivering respectful, person-centred care.
What is health and social care?
Health and social care covers services that support people’s physical health, mental wellbeing, and daily living needs. This includes:
Social care focuses on helping people live independently and maintain their quality of life. You may support:
Older adults
People with disabilities
Individuals with mental health needs
As a caregiver, you play a direct role in improving someone’s daily life, not just their health, but their dignity, comfort, and independence.
Why the care certificate matters to you
The care certificate is not just theory. It prepares you for the real responsibilities of care work.
When you complete it, you will:
Understand your role and responsibilities clearly
Communicate effectively with service users and colleagues
Apply safe practices in real care situations
Deliver care that respects each person’s needs and preferences
Most importantly, it helps you build confidence. You don’t just learn what to do, you learn how to do it properly in real life.
Where it fits in your career
The care certificate is your starting point in health and social care. Many caregivers complete it before moving on to qualifications like NVQ Level 3 Health and Social Care, which develop your skills further and open up career progression opportunities.
If you’re new to the sector, this certificate is your first step into a structured, professional care career.
What Are the 16 Care Certificate Standards? (2026 Update)
The Care Certificate standards define what you must know and do to work safely in health and social care. As of 2025, there are 16 standards, including a new addition covering learning disability and autism.
You must complete all 16 standards before your employer signs off your care certificate.
The 16 Care Certificate Standards (Overview)
The standards cover the core areas of health and social care standards:
Understand your role
Personal development
Duty of care
Equality and diversity
Work in a person-centred way
Communication
Privacy and dignity
Fluids and nutrition
Awareness of mental health, dementia, and learning disability
Safeguarding adults
Safeguarding children
Basic life support
Health and safety
Handling information
Infection prevention and control
Learning disability and autism (new 2025 update)
What these standards mean in real life
Each standard connects directly to what you do every day as a caregiver.
For example:
Communication helps you build trust with service users
Safeguarding teaches you how to recognise and report abuse
Infection control protects both you and the people you care for
The care certificate ensures that every new worker meets the same baseline across the UK. Employers, regulators, and organisations like the NHS rely on these standards to maintain safe, consistent, and high-quality care.
If you want to work in health and social care, these standards form the foundation of everything you will do moving forward.
Duty of Care Explained (What It Means in Practice)
Completing the Care Certificate in a Care Home
Understanding duty of care is one of the most important parts of the care certificate. You will use it every day in your role.
What is duty of care?
Duty of care means you must always act in the best interest of the person you support and take reasonable steps to keep them safe from harm.
Duty of care meaning (simple explanation)
The duty of care meaning is straightforward: You have a responsibility to protect people from harm while supporting their rights, dignity, and independence.
Duty of care definition
A clear duty of care definition is: A legal and professional obligation to provide safe, effective, and compassionate care while avoiding actions that could cause harm.
If you’re starting a role in care, you will almost always need the care certificate. Employers use it to make sure every new worker meets the same health and social care standards before working independently.
You need the care certificate if you are:
A caregiver in a care home or domiciliary (home care) setting
A healthcare assistant in a hospital or community service
A support worker helping people with disabilities or mental health needs
New to health and social care with little or no prior experience
Most employers include the care certificate as part of your induction training.
Why employers expect it
Care providers must show regulators (like the CQC) that their staff are trained and competent. The care certificate helps them prove that.
When you complete it, you show that you can:
Deliver safe care
Follow procedures correctly
Understand your responsibilities
This makes you more employable and trusted in your role.
If you’re applying from overseas
If you plan to work in the UK under a health and care worker visa, employers will often expect you to complete the care certificate shortly after you start work.
While the certificate is not a visa requirement, it:
Helps you adapt to UK care standards
Shows you understand local expectations
Improves your chances of long-term employment
Do experienced workers need it?
If you already work in care and hold qualifications like NVQ Level 3 Health and Social Care, your employer may not require you to complete the full care certificate again.
However, some organisations still use it to:
Standardise training
Refresh knowledge
Ensure compliance with updated standard
How to Get a Care Certificate (NHS & Online)
Foundations of Care Worker Role
You don’t apply for the care certificate like a normal course. You earn it while working in a real care role.
Step-by-step: How to get a Care Certificate NHS online
Start a care job
Join a role such as a caregiver, support worker, or healthcare assistant.
Begin a Care Certificate course
Your employer will enrol you in training. This may include an Elfh Care Certificate programme or another care certificate online provider.
Complete the training workbook
You will study topics based on the Care Certificate standards, including safeguarding, communication, and duty of care.
Apply your learning in the workplace
You must demonstrate what you’ve learned while working with service users.
Get assessed by your employer
A supervisor or assessor will observe your work and confirm your competence.
Receive your certificate
Once you complete all 16 standards and pass assessment, your employer signs off your care certificate.
Important: Online training alone is not enough
You can take a care certificate online course, but this only covers the theory.
To fully achieve the certificate:
You must work in a real care setting
An assessor must sign off your practical skills
This is why many people search for Care Certificate answers, but in reality, you must demonstrate understanding, not just complete quizzes.
Where NHS training fits in
Many organisations use NHS-supported platforms like the Elfh Care Certificate (e-Learning for Healthcare).
This training:
Covers the theoretical part of all standards
Aligns with NHS and Skills for Care guidance
Supports your induction
However, your employer still completes the final assessment in the workplace.
Key takeaway
You get the care certificate by combining training with real work experience, not by completing an online course alone.
This approach ensures you can actually deliver safe, effective care in real-life situations.
Many new caregivers assume they can complete the care certificate online and receive the certificate immediately. In reality, it doesn’t work that way.
What a care certificate online course actually does
A care certificate online course helps you learn the theory behind the Care Certificate standards. It usually includes:
Videos and reading materials
Quizzes or workbook-style questions
Guidance on topics like safeguarding and duty of care
This training builds your knowledge, but it does not mean you have completed the full care certificate.
Why workplace assessment is required
To achieve the care certificate, you must prove that you can apply your knowledge in real situations.
An assessor (usually your manager or supervisor) will:
Observe how you support service users
Check how you communicate and follow care plans
Confirm you meet each of the 16 standards in practice
This step is mandatory. No provider can issue a valid certificate without it.
The truth about “Care Certificate answers”
Many people search for Care Certificate answers online. However:
There are no official answers you can copy
Each employer expects you to demonstrate real understanding
Assessors focus on how you apply knowledge, not just what you write
If you rely only on answers, you won’t pass the practical assessment.
Simple breakdown
Training Type
What You Get
Care certificate online
Knowledge and theory
Workplace assessment
Practical competence
Both combined
Full care certificate
Key takeaway
You can learn the care certificate online, but you must prove your skills in the workplace to achieve it.
This ensures every caregiver can deliver safe, consistent, and high-quality care in real-life settings.
How Long Does It Take and How Much Does It Cost?
Before you start, you’ll want to know how long the care certificate takes and whether you need to pay for it.
How long does the care certificate take?
Most caregivers complete the care certificate within 6 to 12 weeks during their induction.
However, the timeline depends on:
Your employer’s training schedule
Your working hours
How quickly you complete each standard
If you study through a care certificate online course, you can complete the theory in a few hours or days.
But the full certificate takes longer because you must complete workplace assessments.
How much does the care certificate cost?
In most cases, you don’t pay for the care certificate.
Employers usually cover:
Training
Assessment
Certification
If you choose a private Care Certificate course, prices typically range from £15 to £50 depending on the provider.
Free vs paid training
Free options:
NHS-aligned platforms like the Elfh Care Certificate offer free training modules.
Paid options:
Platforms like Caredemy or CPD Online College provide structured courses and certificates of completion.
Remember: paying for a course does not replace workplace assessment.
What affects the total cost?
Even if the course is free, your employer invests in:
Staff time for supervision
Assessment and sign-off
Ongoing training
That’s why most employers include the care certificate as part of your job training.
You can start learning the care certificate through several trusted providers. Most employers will guide you, but it helps to know your options
1. NHS e-Learning (Elfh Care Certificate)
The Elfh Care Certificate (e-Learning for Healthcare) is one of the most widely used platforms in the UK.
It:
Covers all Care Certificate standards
Aligns with NHS and Skills for Care guidance
Offers free, structured online modules
Many care providers use this as part of staff induction.
2. Skills for Care (Official Resources)
Skills for Care provides the official framework, guidance, and materials.
You can access:
Workbooks and guides (care certificate download)
Assessment templates
Employer resources
These materials support both learners and assessors.
3. Online Training Providers
Several platforms offer paid care certificate online courses:
Caredemy
CPD Online College
These providers:
Deliver structured lessons
Provide certificates of completion
Help you prepare for workplace assessment
Useful if you want to learn before starting a job.
Important: Choose the right path
Before enrolling, remember:
Online courses only cover theory
You still need employer assessment to complete the care certificate
Employers may prefer specific training providers
Care Certificate Answers (What You Should Know)
Many new caregivers search for Care Certificate answers online, especially when completing workbooks or quizzes. It’s important to understand how this actually works.
Are there official Care Certificate answers?
No, there are no official Care Certificate answers you can copy and submit.
The care certificate focuses on:
Your understanding
Your ability to apply knowledge
Your performance in real care situations
This means assessors look beyond written responses.
Why copying answers won’t help
Even if you find care certificate answers online:
Your employer will assess you in real situations
You must explain your decisions and actions
You need to show safe and correct practice
If you don’t understand the content, you won’t pass the assessment.
What assessors actually expect
Your assessor wants to see that you can:
Explain your actions clearly
Follow care procedures correctly
Apply the duty of care in real situations
Communicate effectively with service users
They may:
Observe you during care tasks
Ask questions about your decisions
Review your workbook responses
The best way to complete your workbook
Instead of searching for answers, focus on:
Understanding each standard
Using real examples from your work
Writing in your own words
Asking your supervisor when unsure
This approach helps you pass both the written and practical parts.
Care Certificate vs NVQ Level 3 Health and Social Care
Many caregivers ask whether the care certificate is the same as NVQ Level 3 Health and Social Care. They are not the same, they serve different purposes.
What is the difference?
Care Certificate
NVQ Level 3 Health and Social Care
Entry-level training
Advanced qualification
Completed during induction
Completed after gaining experience
Focuses on basic skills and safety
Focuses on deeper knowledge and responsibility
Mandatory (in practice) for new staff
Optional but recommended for career growth
What the care certificate does
The care certificate helps you:
Understand the Care Certificate standards
Learn the basics of health and social care
Work safely under supervision
It prepares you to start your role.
What NVQ Level 3 does
NVQ Level 3 Health and Social Care helps you:
Take on more responsibility
Develop advanced care skills
Progress into senior roles
It builds on what you learned during the care certificate.
Which one should you choose?
If you are new to care:
Start with the care certificate
If you already have experience:
Progress to NVQ Level 3 Health and Social Care
How they work together
Think of it like this:
The care certificate gets you started.
NVQ Level 3 helps you grow your career.
Many employers expect you to complete both over time.
Should You Take the Care Certificate?
If you are new to health and social care, you should complete the care certificate as soon as you start working.
You should take it if:
You are starting your first care role
You want to understand UK care standards
You plan to build a long-term career in care
You may not need it if:
You already hold qualifications like NVQ Level 3 Health and Social Care
You have proven experience and employer sign-off
Most employers will still expect you to complete it.
Conclusion
Starting a career in care can feel overwhelming, especially when you’re expected to understand regulations, responsibilities, and real-life care situations from day one. The care certificate simplifies that journey. It gives you a clear foundation, builds your confidence, and prepares you to deliver safe, compassionate, and person-centred care in real environments.
Whether you’re supporting someone in their home, working in a care facility, or beginning your journey in health and social care, the care certificate helps you do your job properly, not just follow instructions, but truly understand the impact of your actions.
As the sector continues to evolve, one thing remains constant: well-trained caregivers provide better outcomes, build stronger trust, and create safer care environments. The care certificate is where that standard begins.
Need Expert Support Navigating Care Training, Compliance, and Career Progression?
Care Sync Experts supports caregivers, care providers, and healthcare organisations across the UK with clear, practical guidance on care training, compliance, and professional development in health and social care.
From helping new caregivers understand the care certificate, workplace assessments, and duty of care, to guiding organisations on compliance, training frameworks, and operational best practices, our specialists turn complex requirements into simple, actionable steps.
Whether you need support completing your care certificate, improving staff training, or aligning your organisation with Care Certificate standards and CQC expectations, our team delivers tailored guidance designed for real-world care settings.
Build your confidence, strengthen your care delivery, and stay compliant with evolving UK care standards.
Contact Care Sync Experts today to get expert support on care training, compliance, and building a successful career in health and social care.
FAQ
What jobs can you get with a care certificate in the UK?
With a care certificate, you can apply for entry-level roles in health and social care, including: – Care assistant (care homes or domiciliary care) – Support worker (mental health or disability services) – Healthcare assistant (NHS or private settings) – Personal care assistant
These roles allow you to gain experience and progress to higher qualifications like NVQ Level 3 Health and Social Care.
What is the care certificate equivalent to in the UK?
The care certificate is not a formal qualification like a diploma or NVQ. Instead, it is an industry-recognised standard for induction training in health and social care. Think of it as: – A foundation level requirement for new care workers – A stepping stone before moving on to qualifications like NVQ Level 2 or Level 3
It proves competence, not academic achievement.
How much is a Care Worker’s salary in the UK?
Care worker salaries in the UK vary depending on experience, location, and employer. On average: – Entry-level care workers earn £20,000–£24,000 per year – Experienced workers can earn £25,000–£30,000+ – Hourly rates typically range from £10 to £15 per hour – Higher pay is possible with experience, specialist roles, or additional qualifications.
What qualifications do I need to be a care worker in the UK?
You do not need formal qualifications to start a care role, but employers expect you to complete the care certificate during your induction.
To progress in your career, you may need: – NVQ Level 2 or 3 Health and Social Care – Specialist training (e.g., dementia care, safeguarding) – Ongoing professional development
The care certificate is your entry point, while further qualifications help you grow into senior roles.
Cold Weather Payments are £25 government grants that the UK’s Department for Work and Pensions (DWP) pays to eligible low-income households during periods of severe cold weather. The DWP triggers these payments automatically when temperatures in your area drop to 0°C or below for seven consecutive days between 1 November and 31 March.
You do not need to apply. If you qualify through benefits such as Pension Credit or Universal Credit, the DWP sends the cold weather payments directly to your bank account, making it a key DWP extra payment for low-income households during winter.
Key Takeaways
Cold weather payments are £25 for each 7-day period of freezing temperatures between November and March.
The DWP triggers payments automatically based on local weather conditions and postcodes, not individual applications.
Most eligible people receive payment within 14 working days of a cold weather period.
You usually qualify if you receive benefits like Pension Credit, Universal Credit, ESA, or Income Support.
You can check if your area qualifies using the official Cold Weather Payment postcode checker or other tools linked to cold weather payments postcodes.
Scotland does not use this system. Instead, residents receive a fixed winter heating payment Scotland provides each year.
The DWP triggers cold weather payments when the average temperature in your area drops to 0°C or below for seven consecutive days. The system uses both recorded data and forecasts, so you can still receive a payment if a prolonged cold spell is predicted.
The trigger depends on your postcode, not national weather conditions. This means one area can receive a payment while another does not, even within the same region. The DWP links each postcode to a local weather station to track conditions accurately.
For example, if a sub-zero cold snap in Sussex or a wider December freeze UK forecast pushes temperatures below freezing for a full week, the DWP will activate payments for eligible households in those affected postcodes.
This postcode-based system ensures that cold weather payments respond directly to real local weather conditions, helping households manage heating costs during periods of severe cold weather.
How Much Is the Payment and When Will You Be Paid?
The DWP pays £25 for each 7-day period of freezing weather. If multiple cold spells occur, you can receive more than one payment within the same winter.
The DWP usually sends cold weather payments within 14 working days after the cold period ends. You will receive the money in the same bank account as your benefits.
Many people search for “Cold Weather Payment when will it be paid”—the key thing to know is that payment timing depends on when the cold spell finishes, not when it starts.
Payments typically begin during key winter periods such as November 2025, when temperatures first drop, and can continue into late winter, including DWP cold weather payments in March, if cold conditions persist.
If your area experiences repeated freezing conditions, the DWP may issue multiple payments across the season as part of its winter support for low-income households.
Who Qualifies for Cold Weather Payments?
The DWP pays cold weather payments to people receiving specific low-income or disability-related benefits. You must meet both the benefit requirement and the weather condition trigger in your postcode.
Benefits That Qualify
You usually qualify if you receive:
Pension Credit
Income Support
Income-based Jobseeker’s Allowance (JSA)
Income-related Employment and Support Allowance (ESA)
Universal Credit
Support for Mortgage Interest (SMI)
These benefits form the basis of most DWP extra payments for low-income households during winter.
Additional Conditions
In many cases, you must also meet at least one of the following:
You have a child under 5 living with you
You receive a disability premium
You care for someone with a disability
You have limited capability for work
These conditions help the DWP prioritise households most vulnerable to cold weather.
Universal Credit Rules (Important)
If you receive Universal Credit, you typically qualify when:
You are not working or not considered “gainfully self-employed”
Your claim includes a health condition or disability element
You have a young child or disabled child
This is especially relevant during periods like DWP Universal Credit November 2025 payments, when many households rely on additional winter support.
Disability and Additional Support
Households receiving disability-related benefits may also qualify for additional support, such as the winter fuel allowance for disabled individuals, depending on their circumstances.
In short, if you receive qualifying benefits and your area experiences prolonged freezing temperatures, the DWP will automatically issue cold weather payments.
The DWP uses a postcode-based system to decide who receives cold weather payments. Each postcode links to a local weather station, which tracks whether temperatures fall to 0°C or below for seven consecutive days.
You can check your eligibility using the official Cold Weather Payment postcode checker on GOV.UK. Simply enter your postcode to see if your area has triggered a payment.
Here’s how to check:
Go to the official checker tool
Enter your postcode
View whether a payment has been triggered in your area
Many people search for tools like:
DWP cold weather payment postcodes
cold weather payments postcodes
25 cold weather payment postcode checker
These all refer to the same system that confirms whether your location qualifies.
Important: even if you meet the benefit criteria, you will only receive cold weather payments if your postcode area records or forecasts a qualifying cold period.
This ensures the support reaches households actually affected by severe cold weather.
What to Do If You Didn’t Receive a Payment
The DWP sends cold weather payments automatically, but you should act if you believe you qualify and do not receive payment within 14 working days after a cold period ends.
Here’s what you should do:
Check your postcode first
Use the Cold Weather Payment postcode checker to confirm that your area triggered a payment.
Confirm your eligibility
Make sure you receive a qualifying benefit and meet the required conditions.
Contact the right service
If you receive Pension Credit → contact the Pension Service
If you receive Income Support, ESA, or JSA → contact Jobcentre Plus
If you receive Universal Credit → add a note to your online journal
Act quickly
The sooner you report the issue, the faster the DWP can investigate missing cold weather payments.
If your payment is missing, it usually means:
Your postcode did not trigger a payment
Your eligibility changed
Or there was a delay in processing
Taking these steps ensures you do not miss out on a DWP extra payment for low-income households during periods of severe cold weather.
Cold Weather Payments in Northern Ireland and Scotland
Cold Weather Payments vs Other Winter Support
Cold weather payments apply across England, Wales, and Northern Ireland, but the system works differently in Scotland.
Northern Ireland (Same System)
If you live in Northern Ireland, you receive cold weather payments under the same rules as England and Wales.
The DWP uses postcode-based weather data
Payments trigger when temperatures fall below 0°C for 7 days
Eligible households receive £25 automatically
This means cold weather payments Northern Ireland 2026 follow the same structure, timing, and eligibility criteria as the rest of the UK (excluding Scotland).
Scotland (Different System)
Scotland does not use cold weather payments.
Instead, the government provides a fixed annual payment called the Winter Heating Payment.
You receive a flat-rate payment (e.g. £59.75)
The payment does not depend on weather conditions
It supports eligible households regardless of how cold the season gets
This approach ensures households in Scotland receive consistent help without relying on fluctuating cold weather patterns.
Cold Weather Payments vs Other Winter Support
Cold weather payments are only one part of the UK’s winter support system. The DWP also provides other payments that help households manage rising energy costs.
Cold Weather Payments
£25 for each 7-day period of freezing weather
Triggered by postcode-based temperature drops
Paid automatically during periods of severe cold weather
Winter Fuel Payment
A one-off payment of £100–£300
Paid to older people, including those receiving the winter fuel allowance for disabled individuals
Not linked to temperature or cold weather conditions
You receive this payment every winter if you qualify, regardless of how mild or severe the weather is.
Warm Home Discount
A £150 discount on electricity bills
Applied directly to your energy account
Available to eligible low-income households and pensioners
Key Difference
Cold weather payments respond to real-time freezing conditions
Winter Fuel Payment provides guaranteed seasonal support
Warm Home Discount reduces energy bills directly
Many households receive more than one type of support, especially during extreme weather periods or high-cost winters.
Understanding these differences helps you maximise the full range of DWP winter support payments available.
How Cold Weather Payments Help Caregivers (Examples)
Health Effects of Winter Weather
Sarah works as a caregiver supporting an elderly client with limited mobility during a harsh winter. When a December freeze UK forecast turns into a prolonged cold spell, temperatures in her client’s postcode drop below freezing for over a week.
Because her client receives Pension Credit, the DWP automatically triggers a cold weather payment. Within days, the £25 payment arrives in the client’s account.
Sarah uses this support to:
Keep heating on for longer periods
Maintain a safe indoor temperature
Reduce the risk of cold-related health issues
For caregivers, cold weather payments provide more than financial relief—they support safe care delivery during extreme cold weather.
In situations like a sub-zero cold snap, vulnerable individuals rely heavily on consistent heating. These payments help caregivers maintain comfort, prevent illness, and reduce pressure during winter months.
In real terms, cold weather payments ensure that both caregivers and those they support can manage rising energy costs during severe cold weather without compromising care.
Conclusion
Cold weather payments do more than provide £25 during freezing conditions; they give vulnerable households the confidence to stay warm, safe, and supported when temperatures drop. For caregivers, this support plays a critical role in maintaining consistent, high-quality care during winter, especially when energy costs rise and health risks increase.
Understanding how cold weather payments work, when they trigger, who qualifies, and how they interact with other forms of support, helps you make better decisions for yourself or those in your care. Whether you are supporting an elderly person, managing a care service, or navigating benefits for your household, being informed ensures you never miss out on essential winter support.
Need Expert Support Navigating Winter Support, Care Compliance, and Funding Opportunities?
Care Sync Experts supports care providers, families, and healthcare organisations across the UK with clear, practical guidance on accessing government support, understanding benefit entitlements, and maintaining compliance in complex care environments.
From helping caregivers understand how cold weather payments and other DWP support schemes work, to guiding organisations on compliance, funding opportunities, and operational best practices, our specialists simplify complex systems into clear, actionable steps.
Whether you need support navigating winter payments, improving care delivery during cold weather, or aligning your organisation with UK care standards, our team delivers tailored guidance built for real-world care settings.
Support those in your care with confidence while ensuring your organisation stays informed, compliant, and prepared throughout the winter season.
Contact Care Sync Experts today to receive expert guidance on winter support schemes, care compliance, and practical strategies for safer, more effective care delivery.
FAQ
Has DWP triggered Cold Weather Payments for thousands of UK households?
Yes. The DWP regularly triggers cold weather payments during prolonged freezing periods across the UK. In recent winters, the DWP issued over 1.4 million household cold weather payments, showing how widely the scheme supports low-income and vulnerable households during severe cold weather.
Who qualifies for winter heating payment in Scotland?
In Scotland, you qualify for the Winter Heating Payment if you receive certain low-income benefits, such as: – Pension Credit – Universal Credit (with specific conditions) – Income Support or ESA
Unlike cold weather payments, Scotland provides this as a flat annual payment, regardless of temperature. This ensures consistent support throughout winter.
Do people on Universal Credit get heating allowance?
Yes, people on Universal Credit can receive winter support, including cold weather payments, if they meet certain conditions.
You usually qualify if: – You have a health condition or disability, or – You have a child under 5, or – Your claim includes a disabled child element
You may also qualify for other support like the Warm Home Discount, depending on your circumstances.
How do I know if I am entitled to the fuel allowance?
You may be entitled to the Winter Fuel Payment (fuel allowance) if you: – Are above State Pension age – Live in the UK during the qualifying week – Meet residency and benefit conditions
This payment is separate from cold weather payments and does not depend on temperature. Most eligible people receive it automatically, but you can check your eligibility through GOV.UK or by contacting the relevant benefit office.`