Does cold weather make you sick? Not directly. Viruses cause illnesses such as the common cold and flu, not low temperatures themselves. However, cold weather can increase your chances of getting ill because it creates the right conditions for viruses to spread more easily.
During colder months, the air becomes drier, which can dry out the nose and throat. That weakens the body’s ability to trap germs before they enter. Cold weather also pushes more people indoors, where close contact and poor ventilation make it easier for viruses to move from one person to another. So while cold weather does not directly cause infection, it can still play a major role in why winter illness becomes more common.
Quick facts about cold weather and illness
- Cold weather does not directly cause illness, viruses are responsible for infections like colds and flu.
- The idea that does cold weather make you sick is a myth, but cold conditions can increase your risk of exposure to viruses.
- Cold, dry air can irritate and dry out nasal passages, making it easier for viruses to enter the body.
- People spend more time indoors during a UK weather cold snap, which increases close contact and virus transmission.
- You cannot get sick simply from being cold, but prolonged exposure may slightly reduce your body’s defenses.
- Simple habits like handwashing, staying hydrated, and keeping indoor air ventilated can significantly reduce your risk of winter illness.
Does cold weather make you sick myth explained
Many people still believe that cold weather directly causes illness, but this is one of the most common winter health myths. The truth is simple: cold weather alone does not make you sick, viruses do.
This myth likely started because illness rates rise during colder months. People often connect the two and assume temperature is the cause. In reality, several indirect factors explain why more people fall ill in winter.
Cold weather changes how people behave. During colder periods, especially a UK weather cold snap, people stay indoors more often. Enclosed spaces with poor ventilation make it easier for viruses to spread from person to person.
Cold air also affects the body. It can dry out the lining of the nose and throat, reducing the effectiveness of mucus that normally traps germs. This makes it easier for viruses to enter the body, but the cold itself is not the cause of infection.
So when asking, does cold weather make you sick, the accurate answer is: Cold weather increases your risk of exposure and vulnerability, but it does not directly cause illness.
Understanding this distinction helps caregivers and families focus on what truly matters, reducing exposure to viruses, not just avoiding the cold.
RELATED: What Is the Retirement Age in the UK? (2026 Guide for Care Workers & Providers)
Why people get sick more during a UK weather cold snap
Cold weather does not cause illness, but it creates the perfect environment for viruses to spread. During a UK weather cold snap, several factors combine to increase your risk of infection.
- Viruses survive longer in cold, dry air
Viruses such as influenza and the common cold survive longer in cold, low-humidity conditions. Dry air helps virus particles stay airborne for longer periods, making it easier for them to spread between people.
- Indoor crowding increases infection risk
Cold temperatures push people indoors. Homes, care settings, and shared spaces often have limited ventilation, which allows viruses to circulate more easily. This is one of the main reasons illness spreads faster in winter.
- Cold air weakens nasal defenses
Cold air can dry out the lining of the nose and throat. This reduces the effectiveness of mucus, which normally traps viruses before they enter the body. When this barrier weakens, infections become more likely.
- Does cold weather make you sicker or just more exposed?
Cold weather does not necessarily make an infection more severe, but it can increase how often you get exposed to viruses. Repeated exposure, especially in crowded indoor settings, raises the chances of getting sick more frequently.
For caregivers, this matters even more. Vulnerable individuals, such as the elderly or those with existing health conditions, face higher risks during cold periods. Managing indoor environments, improving ventilation, and reducing exposure become essential during winter months.
Can you actually get sick from being cold?
People often ask whether being physically cold can make them ill. The short answer: being cold alone does not cause infection, but it can create conditions that make illness more likely.
Can you get sick from being wet and cold?
You cannot get sick just from being wet and cold. However, staying wet and chilled for long periods can stress the body and lower its ability to fight off viruses, especially if you are already exposed to germs.
Can you get sick from cold air blowing on you?
Cold air blowing on you does not directly cause illness. It may dry out your nose and throat, which can make it easier for viruses to enter, but you still need exposure to a virus to become sick.
Can you get sick from being cold at night?
Sleeping in a cold environment will not directly make you sick. However, poor sleep and prolonged cold exposure can weaken your immune response slightly, which may increase your susceptibility to infections.
Can you get sick from cold feet?
Cold feet alone will not cause illness. However, feeling consistently cold, such as having cold cold feet, can indicate poor circulation or prolonged exposure to low temperatures, which may put extra strain on the body over time.
The key takeaway is clear: Cold conditions do not create illness on their own, but they can make it easier for viruses to take hold if you are exposed.
READ MORE: What Disabilities Qualify for Council Tax Reduction? 2026
Cold, infection, or hay fever symptoms, how to tell the difference
Not every runny nose or sore throat means you are sick. Cold weather can trigger symptoms that feel like illness, while conditions like hay fever can cause similar reactions. Knowing the difference helps you respond correctly and avoid unnecessary treatment.
Cold weather irritation (not an infection)
Cold air can irritate your airways and cause temporary symptoms.
- Mucus: Clear and watery
- Fever: None
- Energy levels: Normal
- Onset: Immediate when exposed to cold air
- Duration: Short (minutes to hours)
- Response: Improves in warm or humid environments
This is your body reacting to temperature, not a virus.
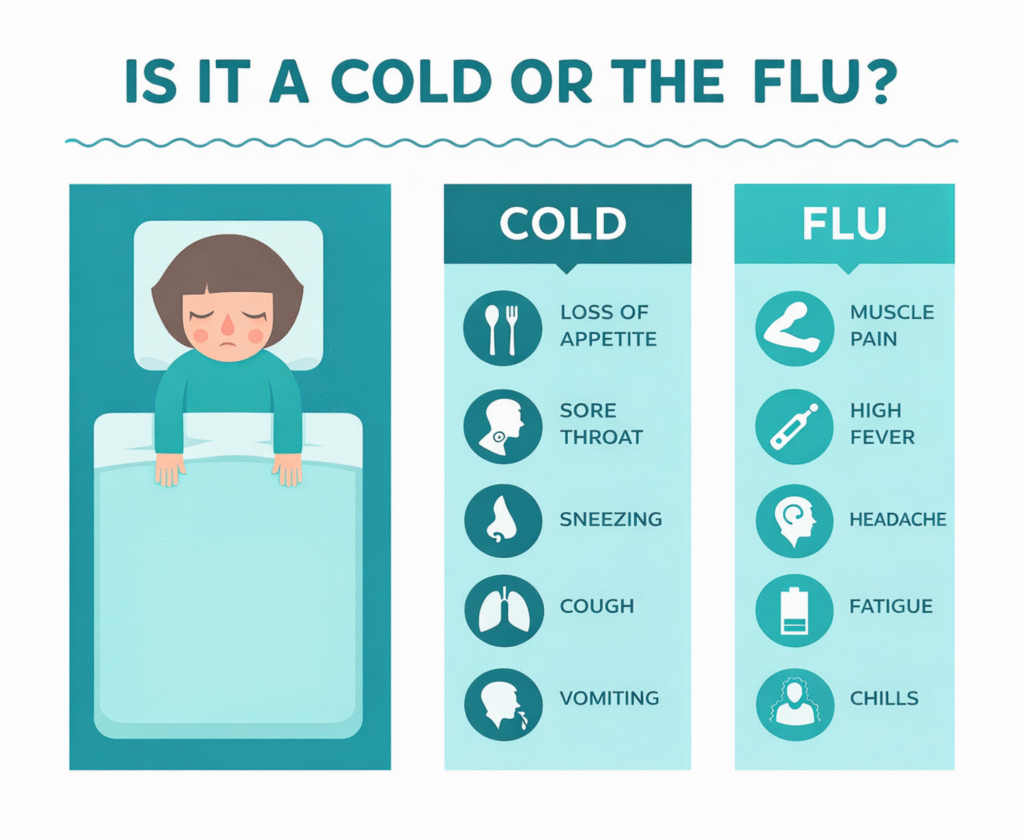
Viral infection (common cold or flu)
A viral infection develops after exposure to germs and usually follows clear stages.
- Mucus: Thick, may become yellow or green
- Fever: Common
- Energy levels: Low, fatigue present
- Body aches: Often present
- Onset: Gradual
- Duration: Several days or longer
These symptoms follow the typical stages of a cold, starting with a sore throat, followed by congestion, and then recovery.
Hay fever (allergic reaction)
Hayfever symptoms can sometimes appear even in colder months, especially indoors due to dust, mould, or pet dander.
- Mucus: Clear and watery
- Fever: None
- Sneezing: Frequent
- Itchy eyes, nose, or throat: Common
- Trigger: Allergens (not viruses or temperature)
- Duration: Persists as long as exposure continues
Many people confuse hay fever with a cold, especially when symptoms overlap.
Quick tip for caregivers
If symptoms improve quickly after warming up or using a humidifier, cold air is likely the cause. If symptoms worsen over time or include fever and fatigue, a viral infection is more likely.
Understanding these differences helps you avoid unnecessary use of sore throat medicine or other treatments when they are not needed, and ensures timely care when symptoms indicate a real infection.
Why caregivers must pay attention during cold weather
Cold weather increases health risks for vulnerable individuals, which makes caregiver awareness essential. While the answer to does cold weather make you sick remains no, the conditions it creates can quickly lead to illness in those with weaker immune systems.
Higher risk for vulnerable groups
Elderly individuals, children, and people with chronic conditions struggle more during cold periods. Their immune systems respond more slowly, and even mild infections can escalate into serious complications such as pneumonia.
Indoor environments increase exposure
Care settings often involve shared spaces. During colder months, reduced ventilation and closer contact increase the spread of viruses. A single infection can quickly affect multiple residents or patients if precautions are not in place.
Cold sensitivity and underlying issues
Some individuals frequently complain, “why am I always cold?” This can signal underlying health conditions such as poor circulation, anemia, or thyroid issues. Caregivers should not ignore these signs, especially during winter.
Monitoring early symptoms
Caregivers should watch for early signs of illness, including:
- Persistent cough
- Fever
- Fatigue or confusion (especially in older adults)
- Changes in appetite or behaviour
Early detection allows faster intervention and reduces the risk of complications.
Practical caregiver actions
- Maintain good indoor ventilation, even during cold weather
- Encourage regular handwashing and hygiene
- Keep individuals warm, especially those with cold cold feet or poor circulation
- Ensure proper hydration and nutrition
- Isolate symptomatic individuals where necessary to limit spread
For caregivers, prevention goes beyond staying warm. It requires actively managing the environment, monitoring symptoms, and reducing exposure risks, especially during periods of increased illness circulation.
SEE MORE: Bereavement Support Payment (BSP) in the UK: Who Qualifies, How Much You Get, and How to Apply
How to stay healthy in cold weather
Staying healthy during colder months requires more than just dressing warmly. While cold weather does not directly cause illness, taking the right precautions can significantly reduce your risk of infection.
Maintain good hygiene
Wash your hands regularly with soap and water, especially after contact with shared surfaces or people who may be unwell. Good hygiene remains one of the most effective ways to prevent viruses from spreading.
Stay hydrated
Drink enough water throughout the day to keep your throat and nasal passages moist. Proper hydration helps your body trap and clear out germs more effectively.
Improve indoor ventilation
Even during a UK weather cold snap, fresh air matters. Open windows when possible or use air circulation systems to reduce the buildup of viruses in enclosed spaces.
Keep warm and avoid prolonged chilling
Dress appropriately for the weather and avoid staying cold for long periods. While being cold alone will not make you sick, it can put stress on the body, especially in vulnerable individuals.
Support your immune system
Focus on:
- Balanced nutrition
- Regular physical activity
- Adequate sleep
These factors strengthen your body’s ability to fight infections.
Manage early symptoms properly
If you develop symptoms like a sore throat, act early. Use appropriate sore throat medicine or sore throat drugs where necessary, stay hydrated, and rest. Early care can prevent symptoms from worsening.
Small daily habits make a big difference. By combining hygiene, proper care, and environmental awareness, you can reduce your risk of winter illness and stay well throughout the colder months.
How to manage symptoms quickly
Act early when symptoms start. Quick, simple steps can reduce discomfort and stop symptoms from getting worse, especially in shared care environments.
Soothe a sore throat
- Drink warm fluids (water, tea, broth) to keep the throat moist
- Use appropriate sore throat medicine or sore throat drugs if symptoms persist
- Try saltwater gargles to reduce irritation and swelling
Early treatment helps prevent progression through the later stages of a cold
Manage nasal congestion
- Use steam inhalation or a humidifier to loosen mucus
- Keep indoor air slightly humid to counteract dry winter air
- Stay hydrated to thin mucus and improve airflow
How to stop hay fever immediately (when allergies are the cause)
Not all symptoms come from infection. If symptoms link to hay fever, act quickly:
- Avoid known triggers (dust, mould, pet dander)
- Use antihistamines as recommended
- Keep windows closed during high pollen exposure (if relevant)
Fast action can relieve hayfever symptoms within hours
Rest and recover
- Prioritize sleep to support your immune system
- Avoid overexertion, which can delay recovery
- Stay warm, but focus more on recovery than temperature alone
Caregiver tip
In care settings, isolate individuals with symptoms where possible and monitor closely. Early management reduces the risk of spread and protects vulnerable individuals.
Quick response makes a difference. Whether symptoms come from a virus, cold air, or hay fever, acting early improves comfort and limits complications.
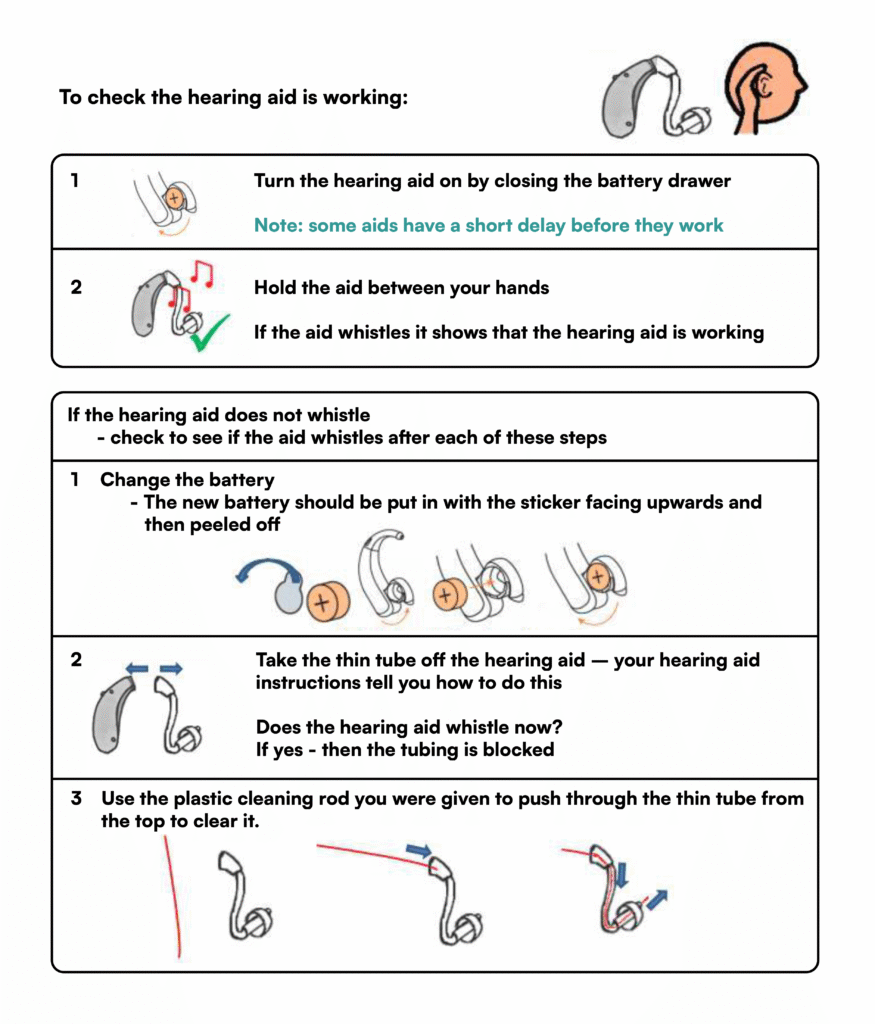
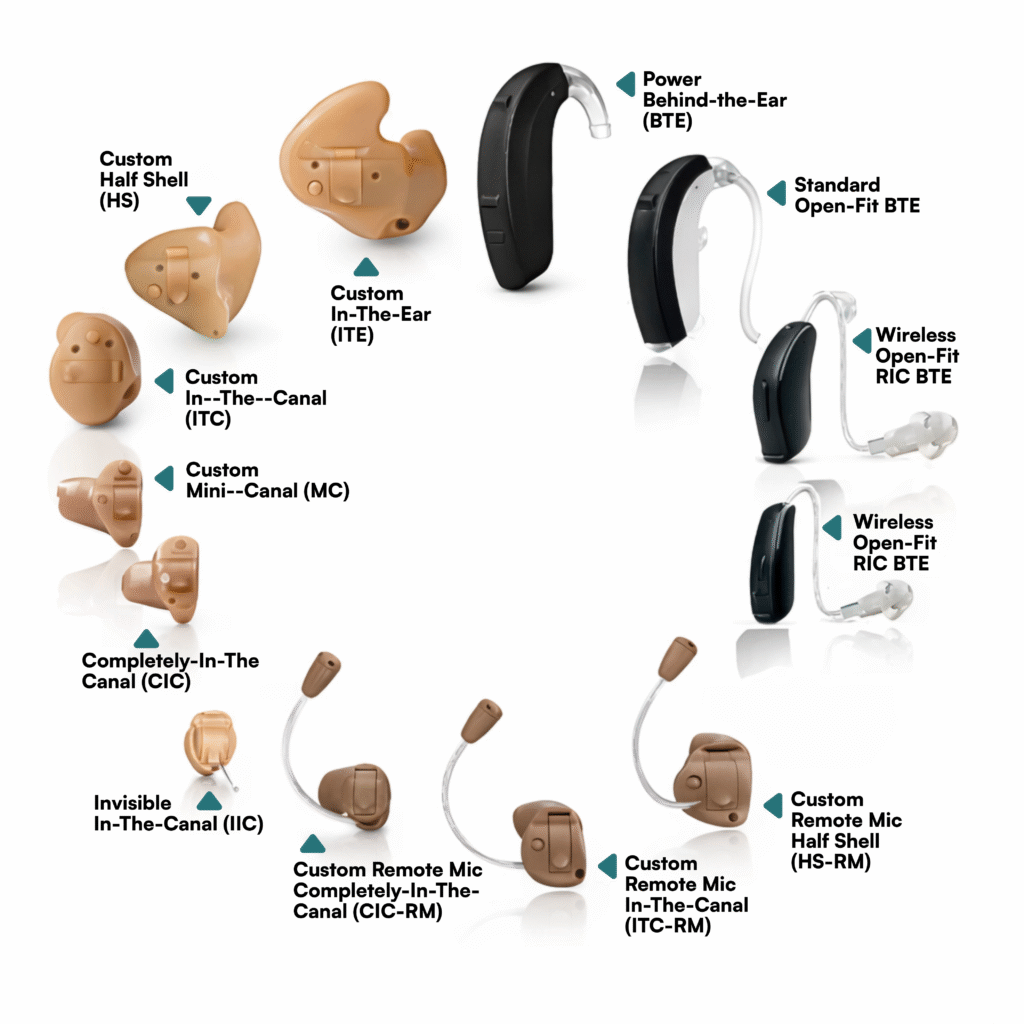
READ: NHS Hearing Aids UK: Cost, Types, Waiting Times, and How to Get One in 2026
When should you see a doctor?
Most winter illnesses resolve on their own, but some symptoms require medical attention, especially for vulnerable individuals. Knowing when to act can prevent complications and ensure proper treatment.
Seek medical advice if symptoms worsen
Contact a healthcare professional if you notice:
- A fever that persists for more than a few days
- Severe or worsening sore throat despite using sore throat medicine
- Difficulty breathing or chest pain
- Ongoing fatigue or weakness that does not improve
- Symptoms that last longer than 10–14 days
These signs may indicate a more serious infection rather than a simple cold.
Watch for high-risk individuals
Caregivers should act quickly if symptoms appear in:
- Older adults
- Young children
- People with weakened immune systems
- Individuals with chronic conditions (e.g. asthma, diabetes, heart disease)
Even mild symptoms can escalate quickly in these groups.
Pay attention to unusual symptoms
Some symptoms may seem minor but still require attention, such as:
- A persistent cough that worsens over time
- Confusion or sudden changes in behaviour (especially in the elderly)
- A blister on lip that is not a cold sore, which may indicate another underlying condition
When symptoms are not improving
If symptoms do not respond to rest, hydration, or basic treatment, it is best to seek professional advice. Early intervention can prevent complications like sinus infections, bronchitis, or pneumonia.
Caregiver reminder
Do not assume all symptoms relate to cold weather. While people often ask, does cold weather make you sick, the real concern is identifying when symptoms go beyond environmental irritation and signal a true infection.
Taking action at the right time protects both the individual and those around them.
Conclusion
Cold weather does not make you sick, but misunderstanding it can. When people assume temperature alone causes illness, they often overlook the real risks: virus exposure, poor indoor ventilation, and weakened natural defenses during colder months.
For caregivers and families, this distinction matters. Recognising the difference between environmental irritation, viral infection, and conditions like hay fever allows for faster, more appropriate responses. It also helps prevent unnecessary treatments while ensuring timely care when symptoms truly require attention.
By focusing on hygiene, early symptom management, and safe indoor environments, especially during a UK weather cold snap, you can significantly reduce the spread of illness and protect those most at risk. Cold weather may set the stage, but informed care and prevention determine the outcome.
Need Expert Support Navigating Health Risks, Compliance, and Care Best Practices?
Care Sync Experts supports care providers, families, and healthcare organisations across the UK with clear, practical guidance on managing seasonal health risks, infection prevention, and regulatory compliance within care environments.
From helping caregivers understand how winter conditions impact illness spread, to guiding organisations on infection control protocols, staff training, and safe care delivery during high-risk periods, our specialists simplify complex health guidance into clear, actionable steps.
Whether you need support improving care quality during colder months, managing infection risks in shared environments, or aligning your practices with UK health and social care standards, our team delivers structured guidance tailored to real-world care settings.
Protect those in your care with confidence while ensuring your organisation stays informed, compliant, and prepared all year round.
Contact Care Sync Experts today to receive expert guidance on seasonal health risks, care compliance, and practical strategies for safer, more effective care delivery.
FAQ
Can breathing in really cold air make you sick?
Breathing in cold air does not directly make you sick, but it can irritate your airways and dry out your nose and throat. This may reduce your body’s ability to trap germs, making it easier for viruses to enter if you are exposed.
What diseases can be caused by coldness?
Cold weather itself does not cause diseases, but it can increase the risk of conditions such as the common cold, flu, and respiratory infections due to higher virus transmission. Extreme cold exposure can also lead to non-infectious conditions like hypothermia and frostbite.
How to protect your lungs in cold weather?
To protect your lungs, caover your mouth and nose with a scarf when outside, stay hydrated, and avoid sudden exposure to very cold air. Maintaining good indoor air quality and avoiding smoke or pollutants also helps keep your lungs healthy.
How can I boost my immune system in the winter?
You can support your immune system by getting enough sleep, eating a balanced diet, staying physically active, and managing stress. Regular handwashing, proper hydration, and good ventilation indoors also reduce your risk of infection during colder months.