If you are asking, “what qualifications do you need to open a care home?”, the honest answer is this: you do not always need formal care qualifications to own one.
You can own a care home as an investor, director or provider, but you must prove that you understand the responsibility that comes with running a regulated care business.
The Care Quality Commission will expect you to act as a fit and proper person, show financial stability, meet legal requirements and put safe systems in place before you provide care.
If you plan to manage the home yourself, you will need the right care experience, leadership skills and usually a recognised management qualification. If you will not manage daily operations, you must appoint a competent Registered Manager.
Opening a care home is not just a property project. You are building a service where people live, receive support and trust your team with their safety, dignity and wellbeing.
A nursing home carries greater responsibility than a residential care home because residents may need regular clinical support. If you want to run a nursing home, you must understand personal care, nursing oversight, medication risks, clinical governance, staffing levels and safe escalation when a resident’s health changes.
You do not have to be a nurse to own a nursing home, but the service must have the right nursing leadership in place. Registered nurses must support residents who need nursing care, and the Registered Manager must show the experience, competence and judgement needed to manage a higher-risk service.
This is where many new owners make a costly mistake. They focus on the building, beds and occupancy plan, but underestimate the clinical responsibility. The Care Quality Commission looks closely at whether nursing homes can keep people safe, meet complex needs and prove that staff have the right skills for the residents they support.
Before you open a care home in England, you must register with the Care Quality Commission. You cannot start providing regulated care first and sort out registration later. The provider, whether an individual, partnership or company, must apply and show that the service can meet the required standards.
Your application must explain the type of care you plan to provide, the location you will operate from, the regulated activities you want to deliver and the people who will manage the service. You also need strong policies, safe recruitment processes, suitable premises, financial planning and clear evidence that you can protect residents from avoidable harm.
CQC registration is not just paperwork. It tests whether your care home has the leadership, systems and culture needed to provide safe, caring and well-led support from the first day residents move in.
Care Certificate, Staff Training and Care Standards
Your care home will only run safely if your staff know what good care looks like in practice. The Care Certificate UK gives new care workers a clear foundation in the behaviours, knowledge and skills expected in adult social care. It covers key care certificate standards such as safeguarding, dignity, privacy, communication, infection prevention, duty of care and person-centred support.
However, the Care Certificate is only the starting point. Your team also needs role-specific training based on the residents you support. This may include dementia care, medication, moving and handling, nutrition, falls prevention, fire safety, mental capacity, end-of-life care and accurate record keeping.
Strong owners build a learning culture early. They do not wait for problems before training staff. They use supervision, spot checks, team meetings and care plan reviews to keep health and social care standards visible every day.
The cost of care homes varies widely because every project starts from a different point. Buying an existing care home, converting a suitable building and building from scratch all carry different costs, risks and timelines. Before you commit, you need to understand both the start-up cost and the monthly running cost.
Your main costs may include property purchase or lease, refurbishment, fire safety work, equipment, furniture, insurance, staff wages, recruitment, training, professional advice, CQC preparation, software, utilities, food, laundry, maintenance and contingency funds.
When people ask, “how much does a care home cost?”, they often focus only on the building. A stronger business owner looks at occupancy, local authority fee rates, private-pay demand, staffing ratios and cash flow. A care home can look profitable on paper and still struggle if wages, agency cover, repairs or low occupancy drain the budget.
Care Home Activities, Resident Experience and Family Trust
Understanding care home costs
Families do not choose a care home because it has beds available. They choose the home that makes them feel their loved one will live safely, comfortably and with dignity. That means your care model must go beyond compliance.
Care home activities play a major role in resident wellbeing. Good activities help people stay socially connected, maintain routines, enjoy hobbies, celebrate identity and reduce loneliness. They also show families that your home sees residents as people, not just care tasks.
If a family asks how to get an elderly person into a care home, they often want more than a placement process. They want reassurance. They want to know the home will communicate clearly, involve them properly and support the person through a difficult transition. A successful care home earns trust before admission and keeps earning it after move-in day.
Care Home vs Care Agency: Do You Need the Same Qualifications?
A care home and a care agency both support people with daily care, but they operate in different ways. A care home provides accommodation and care in one residential setting. A care agency usually sends care workers into people’s own homes to provide visiting care, live-in care or assisted living at home.
The qualification rules also differ by business model. If you ask, “what qualifications do you need to open a care agency?”, the answer is similar in principle: you do not always need formal qualifications to own the company, but you must register with CQC if you provide regulated personal care in England. You also need a competent manager, safe recruitment, staff training, policies, insurance and strong oversight.
So, if you are asking, “what qualifications do I need to open a care company?”, start with the type of service you want to provide. The rules, risks, premises, staffing model and costs will change depending on whether you open a residential care home, nursing home or home care agency.
Final Checklist Before You Open a Care Home
What Qualifications Do You Need to Open a Care Home UK
Before you open a care home, check that your business is ready for both care delivery and regulation.
Choose your care model: residential care, nursing care, dementia care or another specialist service.
Research local demand, competitors, fees and staffing availability.
Prepare a realistic business plan and cash-flow forecast.
Secure funding for start-up costs and early running costs.
Choose premises that can meet safety, accessibility and care requirements.
Understand CQC registration before you spend heavily.
Appoint a competent Registered Manager if you will not manage the home yourself.
Prepare policies, procedures, audits and governance systems.
Recruit staff safely and complete DBS checks.
Build training around the Care Certificate, supervision and residents’ needs.
Plan care home activities, family communication and resident experience from day one.
Get expert support before submitting your CQC application.
A care home succeeds when the owner treats compliance, compassion and commercial planning as one system. Get that right, and you build more than a business, you build a home people can trust.
Opening a care home takes more than funding and a suitable building. You need the right CQC registration, policies, staffing structure, training plan, governance systems and business preparation from the start.
Care Sync Experts can support you with CQC registration preparation, care home compliance, policies and procedures, Registered Manager readiness, mock inspections and wider quality assurance. Whether you plan to open a residential care home, nursing home or care agency, we can help you build a safe, compliant and well-led service.
FAQ
How much does homecare cost per hour in the UK?
Homecare in the UK often costs around £25 per hour, but the final price depends on where the person lives, the type of support they need, the visit length and whether they need specialist care.
Short visits, complex care, overnight support and weekend care may cost more. Families should compare local providers and check whether the person qualifies for local authority funding, NHS support or attendance-related benefits.
Is a care home a good business in the UK?
A care home can be a good business in the UK, but only when the owner understands both care quality and financial discipline. Demand remains strong because many older people need residential, dementia or nursing support.
However, staffing costs, regulation, insurance, utilities, maintenance and occupancy levels can quickly affect profit. The best care home owners do not rely on demand alone. They build a safe service, recruit well, manage cash flow and create a home families trust.
How much does a care home worker earn in the UK?
A care home worker in the UK commonly earns around £20,000 to £25,000 a year, depending on experience, location, employer, shift pattern and responsibility level. Senior care workers, team leaders and staff with specialist skills may earn more.
Pay can also change when employers adjust wages in line with the National Living Wage, local recruitment pressure or additional responsibilities such as medication support, night shifts or dementia care.
Who owns the majority of care homes in the UK?
The majority of care homes in the UK sit within the independent sector, which includes private companies, charities and not-for-profit providers. Private operators play a major role, but no single company owns most care homes.
The market remains mixed, with large groups, smaller independent owners, investors, charities and local authority provision all operating in different parts of the sector.
A care home risk assessment identifies anything that could cause harm to residents, staff, or visitors and sets out practical steps to reduce that risk.
It should cover the whole care environment as well as each resident’s individual needs, including falls, moving and handling, medication, nutrition, dementia-related risks, infection control, fire safety, and safeguarding.
Risk assessments matter because they help care teams prevent avoidable harm before an incident happens. They also give staff clear guidance on what to do, what equipment to use, when to ask for support, and when to review someone’s care.
However, the purpose of a risk assessment is not to remove every risk from a resident’s life. Good care homes use risk assessments to protect people while still supporting dignity, independence, routines, and personal choice.
For example, a resident may want to walk to the garden, make a cup of tea, or take part in an activity that carries some risk. Instead of stopping them automatically, the care team should assess the situation, put sensible controls in place, and help the person enjoy everyday life as safely as possible.
A hazard is anything that could cause harm. A risk is the chance that harm could happen and how serious the outcome could be.
For example, a wet bathroom floor is a hazard. The risk is that a resident could slip, fall, and suffer an injury. A hoist used without the right sling is a hazard. The risk is that the resident or carer could fall or get hurt during a transfer.
In care homes, staff should look beyond obvious hazards such as wet floors, loose carpets, poor lighting, or trailing cables. They also need to consider less visible risks, including medication errors, dehydration, pressure damage, infection, choking, confusion, wandering, or unsafe moving and handling.
Good risk assessment in healthcare examples always link the hazard to the person most likely to be affected. A resident with poor balance may face a higher falls risk than another resident. Someone with dementia may need extra support around exits, routines, or unfamiliar environments.
Once staff understand the hazard and the risk, they can put the right controls in place. That may include clearer routines, equipment checks, extra supervision, staff training, or changes to the environment.
Care homes use different types of risk assessment because residents, staff, visitors, and the building itself can face different risks. A strong care home risk assessment brings these areas together so staff can deliver safe care without losing sight of the person’s choices and routine.
The main types of risk assessment in care include:
Individual resident risk assessments for falls, mobility, moving and handling, nutrition, hydration, skin integrity, medication, personal care, dementia, and behaviour that may place someone at risk.
Environmental risk assessments for slips, trips, poor lighting, unsafe equipment, hot water, infection risks, fire safety, and maintenance issues.
Staff and operational risk assessments for staffing levels, lone working, manual handling, medication procedures, training needs, and emergency response.
Safeguarding and security assessments for abuse, neglect, unauthorised access, missing residents, financial risks, and protecting vulnerable adults.
COSHH assessments for cleaning chemicals, disinfectants, laundry products, and other hazardous substances.
Emergency risk assessments for fire, evacuation, power failure, severe weather, outbreaks, or other incidents that could disrupt care.
Personal care risk assessment examples may include checking whether a resident needs help with bathing, dressing, continence care, eating, or using the bathroom safely. In nursing care, staff may also assess pressure ulcer risk, swallowing difficulties, medication needs, and clinical equipment.
The best assessments do not sit in a folder and gather dust. Care teams should use them every day, share updates clearly, and review them whenever a resident’s needs change.
Risk Assessment in Care Homes Examples
The clearest way to understand risk assessment is to look at everyday care situations. Good assessments do not simply identify a problem; they help carers decide what safe, practical support looks like.
Falls risk: A resident becomes unsteady after a medication change. The team checks their footwear, mobility aid, lighting, hydration, medication timing, and level of supervision. They may add regular checks or encourage the resident to use a walking aid, while still supporting them to move around independently.
Moving and handling: A resident needs help transferring from bed to wheelchair. The assessment should record the correct equipment, sling type, number of carers needed, transfer method, and any pain or mobility issues staff need to consider. This protects both the resident and the carers.
Dementia-related risk: A resident enjoys walking outside but sometimes becomes confused about how to return. Rather than stopping them from going out completely, the care team can agree safer controls such as familiar routes, regular check-ins, a personal alarm, family involvement, or staff support at certain times.
Nutrition and hydration risk: A resident loses weight or struggles to swallow safely. Staff may record food textures, drink preferences, mealtime support, allergy information, weight-monitoring plans, and when to seek clinical advice.
These risk assessment in care homes examples show why care providers need more than generic forms. Each plan should reflect the person’s needs, choices, strengths, and daily routine.
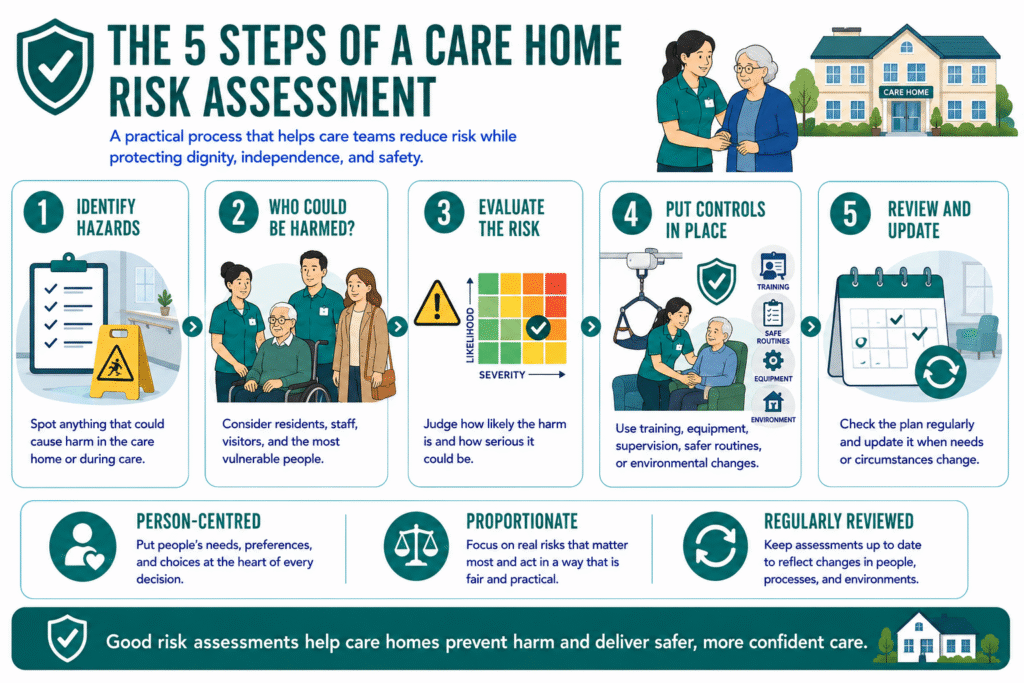
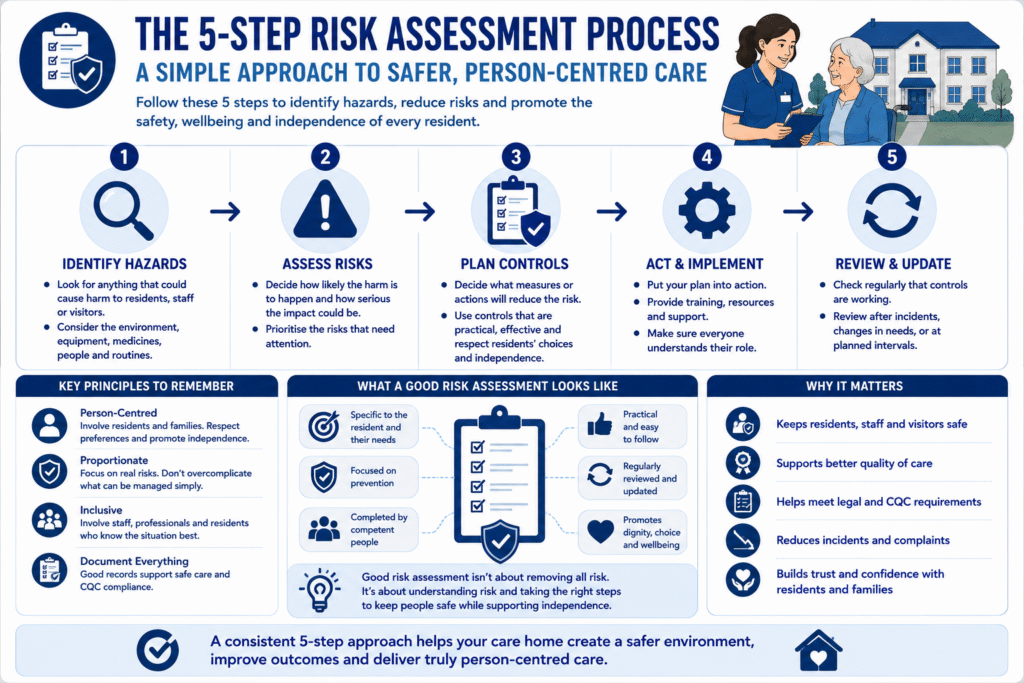
There are five main steps in a risk assessment. Care homes can use this process to spot hazards, protect people, and make sure staff know what action to take.
Identify the hazards Walk through the care home, observe daily routines, speak with staff and residents, and review incident records. Look for anything that could cause harm.
Decide who could be harmed and how Consider residents, staff, visitors, contractors, and the most vulnerable people in the home. A hazard may affect each person differently.
Evaluate the risk and choose controls Decide how likely harm is and how serious it could be. Then put sensible controls in place, such as equipment, training, supervision, safer routines, or environmental changes.
Record findings and put controls into practice Write the assessment clearly. Staff should know what the risk is, what action they need to take, and when they must report concerns.
Review and update the assessment Update the plan when circumstances change. A fall, hospital stay, medication change, infection outbreak, mobility decline, or new equipment may all trigger a review.
So, who should perform a risk assessment? A competent person with the right knowledge should lead it, but good care homes involve carers, managers, residents, families, and relevant health professionals. A risk assessment only works when the people delivering care understand it and follow it consistently.
What Is a Dynamic Risk Assessment?
A dynamic risk assessment happens in the moment when a situation changes and a carer must make a safe decision quickly. Unlike a planned risk assessment, staff do not complete it days or weeks in advance. They use their training, the resident’s care plan, and their professional judgement at the time.
For example, a resident may usually transfer safely from their chair to the bathroom with one carer. One morning, they appear dizzy, weak, or confused. The carer should stop, check what has changed, call for support if needed, and avoid continuing with the usual routine until it is safe.
Dynamic risk assessments also help staff respond to changing situations such as:
A spill on the floor during a busy mealtime
A resident showing signs of distress or agitation
A broken mobility aid or hoist
A sudden deterioration in mobility
A visitor raising a safeguarding concern
A resident refusing care they would normally accept
A good care team does not rush through these moments. Staff pause, assess what has changed, reduce immediate risks, and report the concern so the wider care plan can be reviewed if needed.
Safeguarding, COSHH, and Other Risks Care Homes Must Manage
Care homes need to manage more than falls and moving and handling. They must also protect residents from abuse, neglect, unsafe substances, medication mistakes, infection, and failures in day-to-day care.
Safeguarding in care means protecting people from abuse, neglect, discrimination, avoidable harm, or improper treatment. In practice, this includes listening to concerns, noticing changes in behaviour, recording incidents clearly, and reporting concerns quickly through the right channels.
So, what is safeguarding adults? It is the process of protecting adults who may have care and support needs from harm while respecting their rights, wishes, and involvement in decisions about their lives.
Care homes also need a clear COSHH assessment. COSHH means Control of Substances Hazardous to Health. A COSHH assessment looks at cleaning chemicals, disinfectants, laundry products, and other substances that could harm staff or residents if someone stores, uses, or disposes of them incorrectly.
Other key risks include medication management, infection prevention, fire safety, staffing levels, equipment maintenance, visitor access, and emergency planning. The Care Quality Commission, or CQC, regulates health and adult social care services in England and expects providers to manage these risks safely, consistently, and in a person-centred way.
Why Risk Assessments Matter in Good Care
Common care home risks
Risk assessments protect residents, staff, and visitors, but they should never turn care into a list of restrictions. Good care teams use them to prevent avoidable harm while helping people keep their routines, choices, and independence.
They improve care because they give staff clear guidance. Carers know what support a resident needs, what equipment to use, when to call for help, and what changes they must report. Families also gain confidence when they can see that the home understands the person’s risks and has a plan to manage them.
Risk assessments also support better communication between carers, nurses, managers, families, and health professionals. When everyone works from the same information, the care team can respond earlier to falls, weight loss, confusion, medication changes, pressure damage, or safeguarding concerns.
The Care Certificate also reinforces this approach by covering key areas such as safeguarding, duty of care, dignity, health and safety, fluids and nutrition, infection prevention, and dementia awareness.
The best care home risk assessment does not ask, “How do we remove every risk?” It asks, “How do we help this person live as safely, confidently, and independently as possible?”
Make Risk Management a Strength of Your Care Service
Strong risk assessments protect residents, support carers, and show regulators that your service takes safe, person-centred care seriously.
Care Sync Experts helps care providers build practical systems, strengthen compliance, and create safer services that families and staff can trust.
FAQ
What Are the 5 Risk Assessments?
In a care home, the five most common risk assessment areas are usually: Individual resident risks — such as falls, moving and handling, nutrition, skin integrity, medication, and dementia-related risks. Environmental risks — such as slips, trips, lighting, hot water, fire safety, and unsafe equipment. Staff and operational risks — including staffing levels, lone working, training, and manual handling. Safeguarding and security risks — including abuse, neglect, missing residents, visitor access, and financial harm. Hazardous substance risks — often managed through COSHH assessments for cleaning chemicals, disinfectants, and other substances.
The exact list may vary between homes, but these five areas help providers manage both resident safety and day-to-day care delivery.
What Are 5 Examples of Risk?
Five common examples of risks in a care home include: – A resident falling while walking to the bathroom – A carer injuring their back during a transfer – A medication dose being missed or given incorrectly – A resident choking during a meal – A cleaning chemical being stored where a resident can access it – A risk assessment should identify what could cause the harm, who may be affected, and what controls can reduce the chance or severity of harm.
HSE describes risk assessment as identifying hazards, assessing the risks, controlling them, recording findings, and reviewing the controls.
What Are the 4 Components of Risk Assessment?
A simple risk assessment usually includes four core components: Hazard — what could cause harm Who may be harmed — residents, staff, visitors, or contractors Risk level — how likely the harm is and how serious it could be Control measures — what action will reduce the risk
Many care homes also record who is responsible for each action and when the action must be completed.
HSE templates commonly include existing controls, further actions needed, the responsible person, and deadlines.
What Is a Type 2 Risk Assessment?
“Type 2 risk assessment” is not a standard UK-wide HSE or CQC term. Different providers, local authorities, training companies, and clinical services may use it differently.
In some settings, it can mean a more detailed or specialist assessment completed when a basic assessment identifies a higher level of risk. For example, a resident may need a more detailed moving-and-handling, falls, pressure-care, behavioural, or clinical assessment after an initial concern.
Care homes should avoid relying on the label alone. The important question is whether the assessment clearly identifies the risk, records proportionate controls, names who will act, and sets review triggers.
Part L building regulations are UK rules that set minimum energy efficiency standards for buildings, including how they are designed, heated, insulated, and ventilated. In England, these requirements are explained in Approved Document L, which applies to both new buildings and existing properties undergoing renovation or extension.
For care businesses, Part L UK matters whenever you build, convert, extend, or upgrade a property. Whether you are opening a new care home, converting a house into supported living, or improving an office space, you must meet Part L compliance standards before the building can be approved for use.
The latest updates, often referred to as Part L building regulations 2022, came into effect on 15 June 2022 under the Part L building regulations 2021 framework (with later amendments). These changes introduced stricter requirements to reduce energy use and carbon emissions, as part of the UK’s wider push toward net zero.
In simple terms, building regs Part L ensure that:
Buildings lose less heat through walls, roofs, and windows
Heating systems run efficiently and use less energy
Ventilation systems maintain air quality without wasting heat
Developers and contractors provide clear evidence that work meets required standards
For care providers, this is not just a technical requirement. It directly affects:
resident comfort and safety
energy costs and long-term operating expenses
whether a building can legally open or continue operating
Understanding Part L building regulations early helps care businesses avoid delays, reduce costs, and make smarter decisions when planning or upgrading their services.
Care businesses cannot treat Part L building regulations as a “builder’s problem.” These rules directly affect how you open, run, and scale your service.
Energy efficiency is not just about compliance; it shapes your daily operations.
1. It directly impacts your running costs
Care homes and supported living services operate 24/7. Heating, hot water, and ventilation run constantly.
Poor Part L compliance means:
higher energy bills
inefficient heating systems
long-term financial pressure
Meeting building regs Part L standards helps you reduce energy waste and protect your margins.
2. It affects resident comfort and care quality
Warm, well-ventilated environments are essential in care settings.
Strong insulation and proper Part L building Regulations ventilation improve:
indoor temperature stability
air quality for vulnerable residents
infection control and overall wellbeing
If you get this wrong, you don’t just fail compliance, you compromise care standards.
3. It determines whether your project can open on time
If your building fails Part L UK requirements, building control can delay or block approval.
This can lead to:
delayed service launch
lost revenue
costly redesigns or rework
Many care providers only discover issues late, when fixes become expensive and disruptive.
4. It influences funding, inspections, and reputation
Part L building regulations focus on how a building uses energy and how much heat it loses. In England, Approved Document L explains how to meet these requirements in practice.
For care businesses, this section answers a simple question: What exactly do we need to get right before a building is approved?
1. Two main categories: dwellings vs non-dwellings
Part L UK splits buildings into two groups:
Dwellings (Part L1A / L1B)
Homes where people live independently (e.g. some supported living setups)
Non-dwellings (Part L2A / L2B)
Commercial or institutional spaces (e.g. care homes, offices, clinics)
Most care homes fall under Part L building regulations non dwellings, while supported living can fall under either category depending on layout and level of independence.
Getting this classification wrong can lead to incorrect design, failed approval, and delays.
2. Fabric performance (how well the building retains heat)
Building regs Part L require strong insulation across:
walls
roofs
floors
windows and doors
This is measured using U-values (how much heat escapes).
For care providers, this means:
better temperature control for residents
reduced heating demand
lower long-term costs
3. Heating and hot water systems
Part L building regulations push for more efficient, low-carbon systems.
This includes:
modern boilers or heat pumps
lower flow temperatures
smarter controls
For care environments, heating must balance:
energy efficiency
consistent warmth for vulnerable residents
4. Ventilation and air quality
Part L building Regulations ventilation works alongside other rules to ensure buildings stay healthy as they become more airtight.
This includes:
mechanical or natural ventilation systems
controlled airflow
reduced heat loss while maintaining fresh air
This is critical in care settings, where air quality directly affects health outcomes.
5. Energy modelling and calculations
To prove compliance, developers must use:
SAP (for dwellings)
SBEM (for non-dwellings)
These models calculate:
energy use
carbon emissions
overall efficiency
Care businesses don’t need to run these models, but you must ensure your project team does.
6. Evidence and documentation
One of the biggest changes under Part L building regulations 2022 is stricter proof requirements.
You must provide:
design-stage calculations
as-built performance reports
photographic evidence of construction details
Without this, you cannot demonstrate Part L compliance, even if the building is physically correct.
Approved Document L is not just guidance, it defines what your building must achieve to pass.
For care providers, it covers:
how your building is built
how it performs
how you prove it meets the rules
Understanding this early helps you avoid costly mistakes and ensures your project meets Part L building regulations from day one.
Many care providers assume Part L building regulations only apply to large construction projects. In reality, they affect almost every type of property change in the care sector.
If you run or plan to expand a care business, you will likely trigger Part L compliance at some point.
1. Opening a new care home
New-build care homes fall fully under building regs Part L, usually within the Part L building regulations non dwellings category.
You must meet strict requirements for:
insulation and airtightness
heating system efficiency
ventilation design
full energy modelling and evidence
These projects must align with Part L building regulations 2022, which introduced tighter carbon reduction targets.
2. Converting buildings into supported living
Conversions are common in the care sector, but they come with risk.
If you convert:
a house into supported living
a commercial building into a care facility
You must meet Part L building regulations 2021 standards for existing buildings.
This often means:
upgrading insulation
improving heating systems
meeting minimum energy performance levels
Many providers underestimate how much upgrade work is required.
3. Extending an existing care home
Adding new rooms, wings, or facilities triggers Part L UK requirements.
You must ensure:
the new extension meets current energy standards
the connection between old and new parts does not create heat loss issues
Even small extensions can require significant upgrades to meet compliance.
4. Refurbishing or upgrading existing buildings
Even if you are not building new, Part L building regulations still apply when you:
replace windows or doors
upgrade insulation
install a new heating system
carry out major renovation work
These fall under Part L1B or L2B, depending on the building type.
Many care providers trigger compliance without realising it.
5. Setting up or upgrading a domiciliary care office
Office spaces may seem simple, but they still fall under building regs Part L.
If you:
move into a new office
refit an existing one
upgrade heating or ventilation
You may need to meet energy efficiency standards and provide compliance evidence.
6. Special cases and older buildings
Some care providers operate in older or unique properties, such as a grade 2 listed building.
In these cases:
full compliance may not always be possible
adjustments or alternative approaches may apply
However, you should never assume exemption without expert advice under Part L building Regulations exemptions.
Part L Requirements Care Providers Should Understand Before Starting Work
Before you start any project, you need a clear understanding of what Part L building regulations actually require in practice. This is where many care businesses make costly mistakes, by relying entirely on contractors without understanding the basics.
1. Insulation and building fabric
Building regs Part L place strong emphasis on how well your building retains heat.
You must ensure:
walls, roofs, and floors meet minimum insulation standards
windows and doors limit heat loss
gaps and air leakage are controlled
Better insulation means:
more stable indoor temperatures
improved comfort for residents
lower energy bills over time
2. Heating and hot water systems
Part L building regulations 2022 push for more efficient and lower-carbon systems.
Your project must include:
energy-efficient boilers or heat pumps
properly sized systems for the building
modern controls to manage temperature effectively
In care settings, you must balance efficiency with reliability, residents cannot tolerate inconsistent heating.
3. Ventilation and air quality
As buildings become more airtight, ventilation becomes critical.
Part L building Regulations ventilation ensures:
fresh air circulation
removal of moisture and pollutants
reduced risk of overheating
This often includes:
mechanical ventilation systems
heat recovery systems in some cases
Poor ventilation can lead to:
damp and mould
poor air quality
increased health risks for residents
4. Energy modelling and performance targets
To prove Part L compliance, your project team must complete energy calculations.
These include:
SAP for dwellings
SBEM for non-dwellings
These models assess:
carbon emissions
energy consumption
overall building performance
You don’t need to run these models yourself, but you must ensure they are completed correctly.
5. Evidence and documentation (often overlooked)
One of the biggest shifts in Part L UK is the requirement to prove compliance, not just claim it.
You must provide:
design-stage energy reports
as-built performance reports
photographic evidence of key construction stages
Photos must clearly show:
insulation installation
junction details where heat loss can occur
key building elements before they are covered
Without proper evidence, your building may fail approval, even if the work is correct.
6. Responsibility and coordination
Many care providers assume the builder handles everything.
How Part L Links with Other Rules Care Businesses May Hear About
Part L Building Regulations Compliance
When you plan a care project, you will hear multiple regulations, not just Part L building regulations. This can feel overwhelming, especially if you are not from a construction background.
The key is to understand what each rule covers and how they connect.
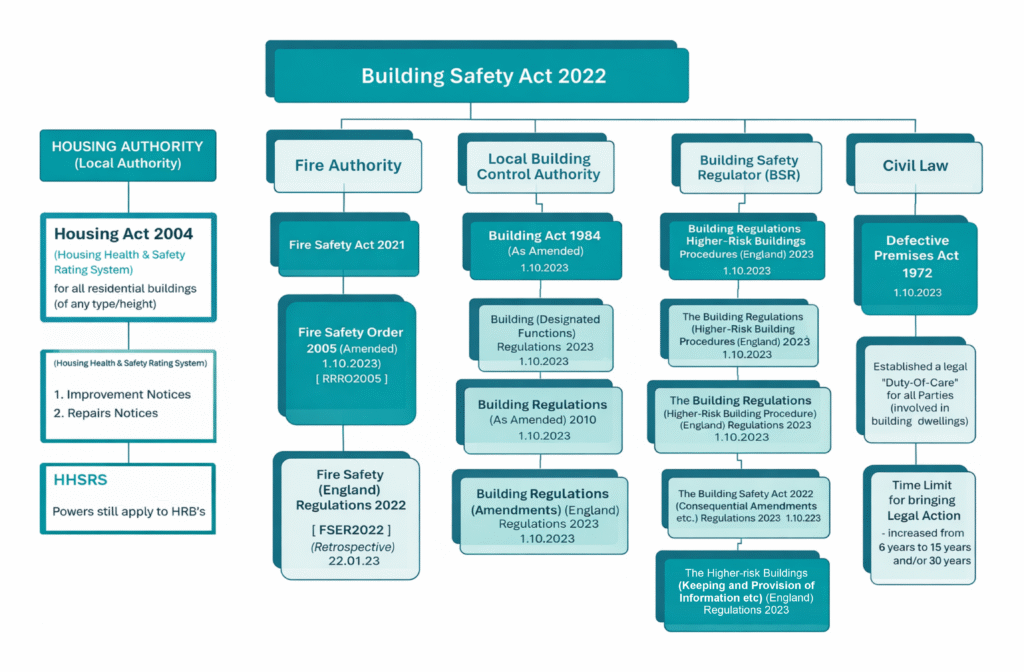
1. Part L vs the Building Safety Act
Part L focuses on energy efficiency. The Building Safety Act and building safety act 2022 focus on safety, accountability, and documentation.
For care providers, this means:
Part L ensures your building performs efficiently
The Building Safety Act ensures your building is safe and properly documented
Both require strong record-keeping and evidence, especially for larger or higher-risk buildings.
2. Part L vs Part M (accessibility)
You will often hear about part m building regulations or approved document m during care projects.
Part L = energy efficiency
Part M = accessibility and usability
In care settings, building regs part m is critical because it covers:
wheelchair access
bathroom layouts
safe movement within the building
You must meet both standards at the same time; one does not replace the other.
3. Part L vs fire safety rules (Part B)
Fire safety falls under:
approved doc b
building regs part b
These rules focus on:
fire detection systems
escape routes
compartmentation
While Part L UK focuses on insulation and airtightness, you must ensure these do not conflict with fire safety design.
4. Other related regulations you may encounter
Depending on your project, you may also hear about:
approved document k (safety around stairs, ramps, and movement)
general building regulations covering structure and ventilation
These do not replace Part L building regulations, but they run alongside them.
5. Why this matters for care providers
Care projects rarely deal with one regulation in isolation.
If you:
build a new care home
convert a property
extend an existing facility
You will need to meet multiple standards at once.
The biggest risk is:
focusing on energy efficiency
while overlooking access, safety, or usability
Part L building regulations form just one part of a wider compliance framework.
For care providers:
Part L = energy performance
Part M = accessibility
Part B = fire safety
Building Safety Act = accountability and safety systems
Understanding how they work together helps you:
avoid design conflicts
prevent costly redesigns
ensure your building meets all approval requirements the first time
Are there any exemptions or special cases under Part L?
Changing Part L Thermal Standards
Many care providers ask whether Part L building regulations always apply in full. The answer is: not always, but exemptions are limited and highly controlled.
You should never assume you qualify for Part L building Regulations exemptions without proper advice.
1. Existing and older buildings
When you upgrade an existing property, Part L allows some flexibility.
For example:
you may not need to upgrade every element to new-build standards
improvements must be “reasonable and practical”
However, you still need to:
improve energy performance where possible
avoid making the building worse
Even partial refurbishment can still trigger Part L compliance requirements.
2. Listed and heritage buildings
Care providers sometimes operate in older or historic properties, such as a grade 2 listed building.
In these cases:
strict upgrades (like replacing windows or external insulation) may not be allowed
heritage protection can limit what changes you can make
However:
you must still improve energy efficiency where it does not damage the building’s character
This often requires:
specialist advice
tailored solutions
3. Technical and practical limitations
Some buildings cannot meet full modern standards due to:
structural limitations
space constraints
compatibility with existing systems
In these situations:
alternative measures may be accepted
compliance focuses on “reasonable improvement” rather than perfection
4. What does NOT count as an exemption
Care providers often misunderstand this.
You are not exempt just because:
the building is old
the project is small
you are only making minor changes
you are leasing the property
If your work affects energy performance, building regs Part L will likely apply.
5. Why exemptions still require documentation
Even when flexibility applies, you must:
justify your approach
document decisions
show why full compliance was not possible
Building control will still expect:
clear reasoning
supporting evidence
Part L building regulations rarely offer full exemptions.
In most cases:
you must comply fully
or improve performance as far as reasonably possible
Care providers who assume they are exempt often face:
delays
redesign costs
compliance issues during approval
The safest approach is simple:
Always check early, plan properly, and treat Part L compliance as part of your core project strategy.
Many care providers run into problems with Part L building regulations, not because the rules are unclear, but because they get involved too late or rely on the wrong assumptions.
Avoiding these mistakes can save you time, money, and project delays.
1. Treating Part L as the builder’s responsibility
Many providers assume the contractor will “handle compliance.”
In reality:
you own the project
you remain responsible for Part L compliance
poor coordination can still lead to failure
You need visibility from design to completion.
2. Signing a lease or buying a property without checking requirements
This is one of the most expensive mistakes.
Care providers often:
secure a building first
check building regs Part L later
This can lead to:
unexpected upgrade costs
delays in opening
redesign of heating, insulation, or ventilation systems
Always assess Part L building regulations before committing to a property.
3. Assuming only new builds are affected
Many providers think Part L UK only applies to new construction.
In reality, it also applies when you:
refurbish
extend
replace key building elements
Even simple upgrades can trigger compliance requirements.
4. Ignoring ventilation when improving insulation
Improving insulation without considering Part L building Regulations ventilation creates serious problems.
This can lead to:
poor air quality
damp and mould
overheating
Energy efficiency must always balance with ventilation.
5. Underestimating documentation and evidence
Some providers focus on the physical build but forget about proof.
Under Part L building regulations 2022, you must provide:
energy calculations
as-built reports
photographic evidence
Without this, your project may fail, even if everything is installed correctly.
6. Leaving compliance too late in the project
If you only think about Part L during construction, you are already at risk.
Late changes can mean:
redesigning systems
replacing materials
increased costs
The best projects consider compliance at the design stage.
7. Not involving the right professionals early
Successful projects require:
energy assessors
consultants
experienced contractors
If you delay bringing them in:
mistakes go unnoticed
compliance gaps increase
Bottom line
Most Part L building regulations issues come down to timing and awareness.
Care providers who:
plan early
ask the right questions
stay involved
Avoid delays, reduce costs, and achieve smooth approvals.
Those who don’t often face:
rework
compliance failures
delayed service launches
Final takeaway for care providers
Part L building regulations are not just a technical requirement, they directly shape how your care business operates, grows, and delivers safe environments.
If you plan to:
open a new service
convert a property
extend or refurbish a building
You must consider Part L compliance from the very beginning.
Care providers who approach Part L UK correctly:
control energy costs
create comfortable, healthy environments for residents
avoid delays during approval
protect their investment
Those who ignore it often face:
unexpected upgrade costs
failed inspections
delayed openings
The simple rule to follow
Treat building regs Part L as a business priority, not just a construction detail.
If you:
check requirements early
work with the right professionals
plan for both performance and evidence
You will meet compliance smoothly and avoid costly mistakes.
One final perspective
Energy efficiency is no longer optional. It sits at the centre of modern care delivery.
Understanding Part L building regulations helps you:
build smarter
operate more efficiently
deliver better care environments
And in a sector where comfort, safety, and sustainability matter every day…
That is a competitive advantage.
Need Expert Support Navigating Building Compliance and Care Facility Requirements?
Care Sync Experts supports care providers, care home operators, and healthcare organisations across the UK with clear, practical guidance on regulatory compliance, property requirements, and operational readiness.
From helping you understand Part L building regulations, energy efficiency standards, and building compliance requirements, to guiding you through property conversions, refurbishments, and service setup, our specialists turn complex regulations into simple, actionable steps.
Whether you are opening a new care home, converting a property into supported living, upgrading your facilities, or ensuring full Part L compliance alongside CQC expectations, our team delivers tailored support designed for real-world care environments.
Plan smarter, avoid costly mistakes, and ensure your care premises meet all regulatory standards from day one.
Contact Care Sync Experts today to get expert support on building compliance, care facility setup, and navigating UK care regulations with confidence.
FAQ
Is Part L law in the UK?
Yes. Part L building regulations form part of the Building Regulations in England and are legally enforceable. While Approved Document L provides guidance on how to meet the requirements, the underlying regulation itself is law.
If a care provider or developer fails to meet Part L compliance, building control can: – refuse approval – require corrective work – issue fines or enforcement action In simple terms: you must comply with Part L to legally complete and use a building.
What are carbon emission targets in Part L?
Part L building regulations 2022 introduced stricter carbon reduction targets as part of the UK’s journey toward net zero.
For new buildings: – new homes must reduce carbon emissions by around 30% compared to previous standards – future standards aim for 75–80% reductions by 2025
For care providers, this means: – more efficient heating systems – better insulation – lower overall energy use
These targets directly influence design, costs, and long-term energy performance.
What is the 10 year rule for listed buildings?
The “10-year rule” is often misunderstood. It does not automatically exempt buildings from regulation, including Part L building regulations.
In planning terms, it generally refers to situations where: – unauthorised work may become lawful after 10 years if no enforcement action is taken
However, for buildings such as a grade 2 listed building: – separate listed building consent rules still apply – energy upgrades must balance compliance with heritage protection
Care providers should always seek professional advice; never assume older or listed buildings are exempt from compliance requirements.
What are the 7 stages of construction?
Understanding the construction process helps care providers manage Part L compliance effectively. The typical stages are: – Planning and feasibility – Design and approvals – Procurement and contractor selection – Site preparation – Construction – Inspection and compliance checks – Completion and handover
Part L building regulations apply across multiple stages, especially: – design (energy modelling and specifications) – construction (installation quality) – completion (evidence and certification)
Getting involved early in these stages helps care businesses avoid delays and ensure smooth approval.
If you’re do dementia sufferers have to pay care home fees, the answer is yes. Many dementia sufferers do have to pay care home fees in the UK, because dementia care is usually classified as social care rather than medical care. This means the cost of a dementia care home is typically assessed through a financial (means) test carried out by the local authority.
If a person’s savings, income, or assets exceed certain thresholds, they usually have to pay for their own care home fees, either fully or partly. In England, for example, people with more than £23,250 in assets are generally expected to fund their own care.
However, some people with dementia may receive financial support or fully funded care, depending on their circumstances.
Self-funding is common. Many families pay privately for dementia care homes when savings or property exceed the means-test threshold.
Local authorities may contribute. If assets fall below the upper threshold, the council may help with care home fees.
NHS Continuing Healthcare (CHC) may cover the full cost of care if the person’s needs are primarily medical rather than social.
NHS-Funded Nursing Care (FNC) may pay a weekly contribution if the person lives in a nursing home and needs care from registered nurses.
Because of these rules, dementia care home costs in the UK vary widely. Some families pay the full price of long-term care, while others receive partial or full funding depending on their financial situation and health needs.
Understanding how the system works is the first step toward finding help with care home fees for dementia patients and planning the right level of support.
Why dementia care home costs in the UK are often high
Many families feel shocked when they first see dementia care home costs in the UK. Unlike standard residential care, dementia care requires specialist support, higher staffing levels, and a secure environment, all of which increase the overall cost of care homes.
People living with dementia often need help throughout the day and night. Care teams support residents with memory loss, confusion, mobility problems, and changes in behaviour. As the condition progresses, care homes may provide enhanced dementia care, which includes:
24-hour supervision and support
Staff trained specifically in dementia care
Secure layouts to prevent wandering
Structured routines and therapeutic activities
Specialist nursing care for complex health needs
These additional services make dementia care homes more resource-intensive than many other forms of residential care.
Location also plays a major role in the cost of an old people’s home. Care homes in cities or areas with higher staffing costs often charge significantly more than homes in rural regions. Facilities that provide specialist dementia units, private rooms, or advanced medical care may also charge higher fees.
For caregivers searching online for dementia care homes near me or a care home for dementia near me, the price can vary dramatically depending on the level of support required. Families often discover that dementia care involves not just accommodation but round-the-clock professional care, which is why the price of long-term care can feel overwhelming at first.
Understanding these factors helps families prepare for the financial side of dementia care and explore available funding options before making long-term decisions.
The cost of care homes for dementia in the UK varies widely depending on the type of care, the location, and the level of support required. However, most families can expect dementia care to cost more than standard residential care, because specialist support and supervision are often needed.
On average, weekly dementia care home costs in the UK are approximately:
Residential dementia care: around £1,200 – £1,500 per week
Nursing dementia care: around £1,400 – £1,700 per week
These figures represent the typical price of long-term care, but the final cost depends on several factors.
What affects the cost of care homes?
Several factors influence how much families pay for care home fees, including:
Location: Care homes in London and major cities often charge more than those in smaller towns.
Level of care required: Residents who need specialist nursing or behavioural support may face higher costs.
Facilities and services: Private rooms, specialist dementia units, and enhanced dementia care programs can increase fees.
Availability of care homes: In some areas, limited supply means higher prices.
For families searching online for “dementia care homes near me”, prices can vary significantly even within the same region. Some homes focus on standard residential support, while others offer specialist dementia care homes with trained staff and secure environments designed specifically for memory conditions.
Because of these variations, the cost of an old people’s home or dementia care home can differ greatly from one provider to another. This is why many families first research local options before deciding whether to fund care privately or apply for financial support.
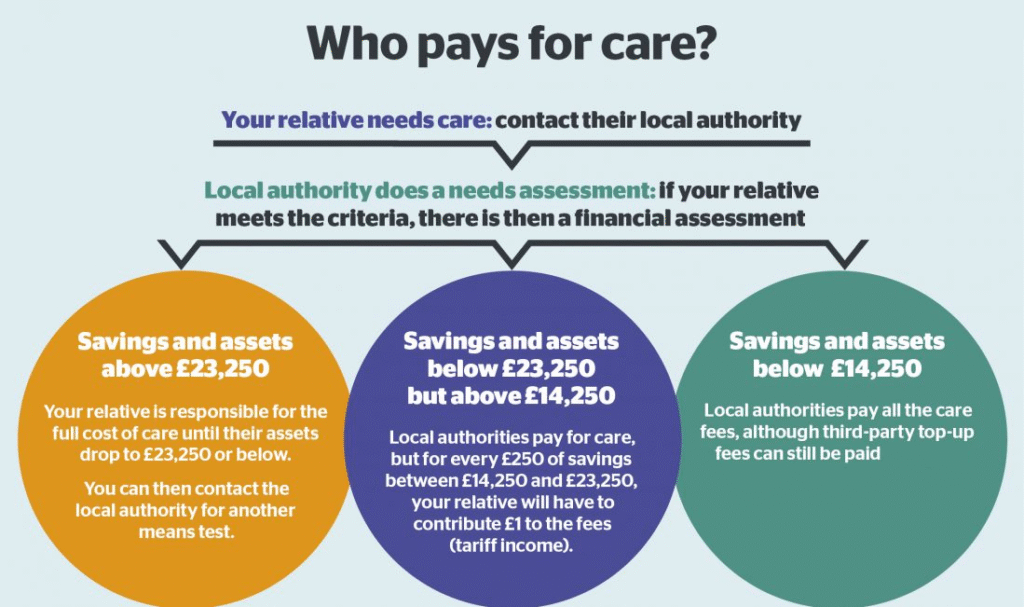
Who pays dementia care home fees in the UK?
do dementia sufferers have to pay care home fees 2026
In most cases, who pays care home fees depends on a financial (means) assessment carried out by the local authority. This assessment looks at the person’s income, savings, and assets to determine whether they must pay for their care themselves or qualify for financial support.
Many people with dementia end up paying some or all of their care home fees, particularly if they have savings or property above the government thresholds.
The financial assessment explained
Before funding any care placement, the local council will usually complete two assessments:
Needs assessment – Determines what type of care the person requires (home care, residential care, or nursing care).
Financial assessment – Calculates how much the person should contribute toward the cost of care homes.
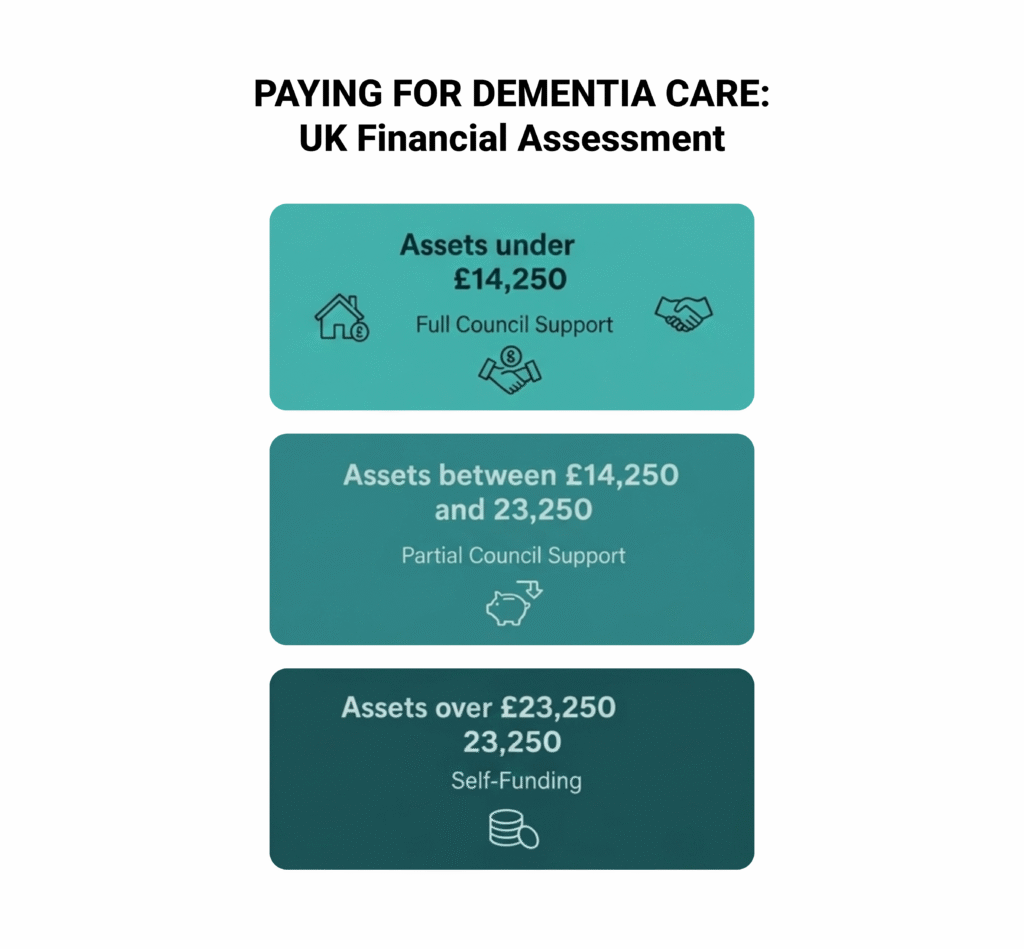
In England, the main capital limits currently work as follows:
Over £23,250 in assets: The person normally pays the full dementia care home costs UK privately (self-funding).
Between £14,250 and £23,250: The person contributes toward care costs, and the local authority may help pay the rest.
Below £14,250: The local authority usually covers most care costs, although income such as pensions may still contribute.
Assets considered in the financial assessment can include:
Savings and investments
Property (in some cases)
Pensions or regular income
However, the value of a home may not always be included in the assessment. For example, if a spouse or dependent relative still lives in the property, the council may disregard its value.
Local authority funding for care
If someone qualifies financially and meets eligibility criteria, the council may provide local authority funding for care in your own home or help cover the cost of a residential placement.
Families often start researching how to get help with care home fees once they understand the outcome of the financial assessment. The council may either arrange the placement directly or provide a personal budget to support the person’s care needs.
Understanding how the financial assessment works can help families plan ahead and explore the options available for help with care home fees for dementia patients.
Is there free care home funding for dementia patients?
Many families ask whether there is free care home funding for dementia patients in the UK. In most situations, dementia care is not automatically free, because the system treats it primarily as social care rather than healthcare. However, some people with dementia may qualify for funding that covers part or all of their care home fees.
Two NHS funding routes can help reduce dementia care home costs in the UK.
NHS Continuing Healthcare (CHC)
NHS Continuing Healthcare is a package of care fully funded by the NHS. If someone qualifies, the NHS pays the full cost of care, including accommodation and nursing support in a care home.
Eligibility does not depend on savings or assets. Instead, assessors decide whether the person has a “primary health need.” This means their care needs mainly involve medical supervision rather than personal support.
Some people with advanced dementia qualify for CHC when they experience complex needs such as:
Severe cognitive impairment
High levels of behavioural distress
Complex mobility problems
Significant medical supervision needs
Although families sometimes assume dementia automatically qualifies for CHC, this is not always the case. Each person must go through a detailed assessment conducted by healthcare professionals.
For those who meet the criteria, CHC effectively provides free care for dementia patients in the UK, because the NHS covers the full cost of care.
NHS-Funded Nursing Care (FNC)
If someone lives in a nursing home but does not qualify for CHC, they may still receive NHS-Funded Nursing Care.
Under this scheme, the NHS pays a weekly contribution toward the nursing element of care. The payment goes directly to the care home and helps reduce the overall care home fees families must pay.
FNC does not cover accommodation or personal care costs, but it can still provide meaningful financial support for people living in specialist dementia care homes that require registered nursing staff.
Understanding these funding options helps families determine whether they can access help with care home fees for dementia patients, particularly when dementia progresses, and care needs become more complex.
Are next of kin responsible for care home fees?
Pay for Dementia Care-Uk Financial Assessment
Many families worry that they might personally inherit the care home fees of a loved one with dementia. In most cases, next of kin are not legally responsible for paying care home fees.
The person receiving care usually remains responsible for their own dementia care home costs in the UK. Local authorities or the NHS may contribute depending on the outcome of the needs and financial assessments, but family members do not automatically become liable for the bill.
However, there are a few situations where a relative may agree to pay part of the cost.
When families may contribute to care home fees
A family member may become financially involved if they choose to:
Sign a contract with the care home agreeing to pay part of the fees
Provide a third-party top-up payment if they select a more expensive home than the local authority normally funds
Manage finances on behalf of the person through Lasting Power of Attorney
For example, if a council agrees to fund care up to a certain amount but the family prefers a more expensive care home for dementia near me, they may choose to pay the difference as a top-up.
What families should understand
In most cases:
Next of kin are not automatically responsible for care home fees.
The financial assessment focuses on the assets and income of the person receiving care.
Families should carefully review any agreements before signing documents with a care home.
Understanding this distinction can reduce anxiety for caregivers who already face emotional and practical challenges when supporting someone living with dementia.
Not every person with dementia needs to move into a care home immediately. Many families first explore care at home, especially in the early or moderate stages of dementia. Understanding home care services cost can help caregivers decide whether staying at home is a practical alternative.
How much does home care cost per hour in the UK?
The cost of home care services depends on the level of support required and the region where you live. On average:
Home care services: around £20–£35 per hour
Live-in carer cost: roughly £900–£1,600 per week depending on care needs
Private nursing care: higher costs if medical support is required
Families often search questions such as “how much does home care cost per hour UK” or “how much does a home nurse cost” when deciding whether home care might be more affordable than residential care.
When home care may work better
Home care can be a suitable option when a person with dementia:
Can still live safely in familiar surroundings
Needs help with daily tasks such as washing, dressing, or medication
Benefits from routine and familiar environments
In some situations, the local authority may also provide local authority funding for care in your own home after completing a needs and financial assessment.
When residential care becomes necessary
As dementia progresses, some people eventually require 24-hour supervision or specialist dementia support. At that stage, families may start exploring dementia care homes near me or a care home for dementia near me that offers structured care and specialist staff.
Understanding the differences between home care and residential care helps families make informed decisions about the cost of care homes, the price of long-term care, and the level of support their loved one truly needs.
How to get help with care home fees for dementia patients
Many families feel overwhelmed when they first learn about dementia care home costs in the UK. The good news is that several funding routes may help reduce or cover care home fees, depending on the person’s financial situation and care needs.
If you are wondering how to get help with care home fees, the process usually begins with two important assessments arranged through your local authority.
1. Request a care needs assessment
Start by asking your local council for a care needs assessment. A trained professional will evaluate the person’s condition and decide what level of support they require. This assessment determines whether the person needs:
Home care support
Specialist dementia care
A residential or nursing care home
The results help the council decide what type of support they can provide.
2. Complete a financial assessment
If the person needs residential care, the council will then carry out a financial (means) assessment to determine who pays for the care.
The assessment considers:
Savings and investments
Income, such as pensions
Property ownership
Other financial assets
Depending on the results, the local authority may contribute toward the cost of care homes, or the person may need to self-fund their care.
3. Ask about NHS funding options
Families should also ask for an assessment for NHS Continuing Healthcare (CHC) if the person has complex health needs. If approved, CHC can cover the full cost of care, including accommodation in a care home.
If CHC is not granted but the person lives in a nursing home, they may still qualify for NHS-Funded Nursing Care, which contributes toward the nursing portion of care home fees.
4. Check benefits and financial support
Some people with dementia may qualify for additional financial help, including:
Attendance Allowance
Personal Independence Payment (PIP) for people under pension age
Pension Credit
Council tax reductions for severe mental impairment
These benefits can help cover daily expenses and reduce the overall price of long-term care.
5. Explore deferred payment schemes
If the person owns a home but does not want to sell it immediately, the local authority may offer a deferred payment agreement. This allows care fees to be paid later, usually when the property is eventually sold.
Understanding these steps helps families access help with care home fees for dementia patients and navigate the financial side of care with more confidence.
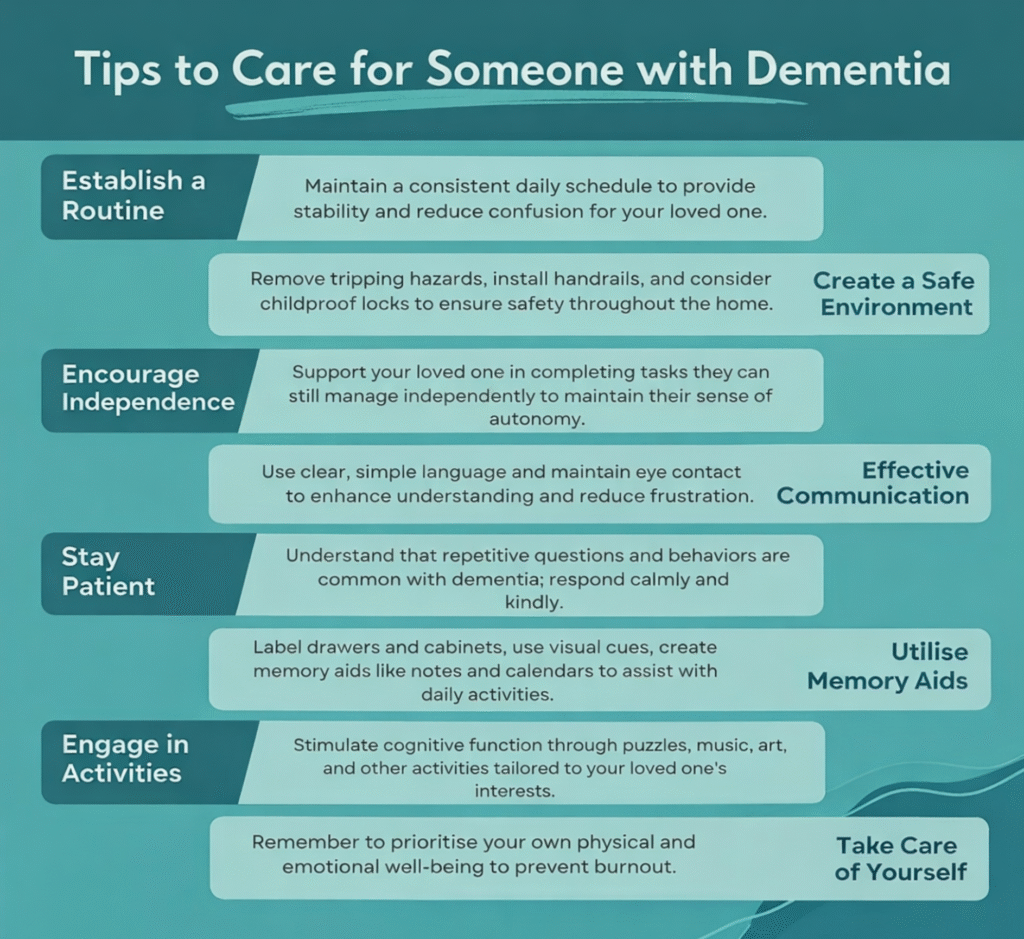
Tips for caring parent or loved ones with dementia at home
When dementia progresses, and care needs increase, many families begin searching online for dementia care homes near me or a care home for dementia near me. Choosing the right home can feel overwhelming, but taking a structured approach can make the process easier.
Start with local authority directories
Your local council usually keeps a list of approved providers and can help you identify government funded care homes near me that meet required standards. If the local authority funds part of the placement, they may suggest care homes that work within their funding arrangements.
However, families can still explore other dementia care homes if they prefer a different location or service. In some cases, this may involve paying a top-up fee if the chosen home costs more than the council normally covers.
Check care quality ratings
Before choosing a care home, review the inspection ratings from the relevant regulator:
Inspection reports can reveal important details about safety, staffing levels, and the quality of dementia care provided.
Visit care homes in person
Whenever possible, visit several dementia care homes near you before making a decision. Pay attention to:
Staff interactions with residents
Safety and cleanliness
Activities designed for people with dementia
Secure layouts for residents who may wander
Many homes offer specialist enhanced dementia care, including memory-friendly environments, trained staff, and structured daily routines.
Consider care needs and future progression
Dementia is a progressive condition, so it is important to choose a home that can support increasing care needs over time. Some homes provide both residential and nursing care, which allows residents to remain in the same environment as their condition changes.
Taking time to research and visit care homes for dementia near you helps families make confident decisions and ensures their loved one receives the level of care and support they truly need.
Key facts about dementia care home fees
If you are supporting someone with dementia, understanding how care home fees work can make the financial side of care much less confusing. The most important points families should remember include the following:
Many people with dementia pay for their own care. Dementia care is usually treated as social care, which means funding depends on a financial assessment rather than being automatically covered by the NHS.
Local authorities may help with the cost of care homes. If a person’s savings and assets fall below the capital thresholds, the council may contribute toward their care.
NHS funding is sometimes available. People with complex medical needs may qualify for NHS Continuing Healthcare, which can cover the full cost of care.
NHS-Funded Nursing Care may reduce costs. If someone lives in a nursing home but does not qualify for full NHS funding, the NHS may contribute a weekly amount toward the nursing element of care.
Home care can be an alternative in earlier stages. Some families explore options such as live-in carers or hourly support before moving to residential care.
Understanding these key facts can help families plan ahead, explore help with care home fees for dementia patients, and make informed decisions about the best care options for their loved ones.
New rules for care home payments in the UK (2026 update)
Families often ask whether the government has introduced new rules for care home payments that could reduce the price of long-term care. The UK government has discussed several reforms to the social care system in recent years, but the way care home fees work largely remains the same for most families.
The proposed care cost cap
A major reform previously planned was a cap on lifetime care costs, which would have limited how much individuals pay for personal care over their lifetime. The proposed cap was set at £86,000.
However, the government later delayed these reforms, meaning the current funding system still relies mainly on the means-tested financial assessment used by local authorities.
What this means for families today
For now, most people entering a care home will still follow the existing system:
People with assets above the upper capital limit usually self-fund their care.
Those with fewer assets may receive local authority support.
NHS funding remains available through Continuing Healthcare or NHS-Funded Nursing Care for those who qualify.
Because policy changes can happen over time, families should always check the latest government guidance or speak with their local authority before making long-term financial decisions about care.
Understanding these rules can help caregivers plan ahead and better prepare for the cost of care homes or specialist dementia care homes in the future.
Conclusion
Understanding whether dementia sufferers have to pay care home fees can feel confusing at first, especially when families face emotional and financial pressure at the same time. In the UK, dementia care is usually treated as social care, which means many people pay for some or all of their care home fees depending on their financial situation.
The amount someone pays depends on several factors, including their savings, property, and the outcome of a local authority financial assessment. Some people qualify for support from the council, while others may receive NHS funding through Continuing Healthcare or NHS-Funded Nursing Care if their needs are primarily medical.
Because dementia care home costs in the UK can be significant, families benefit from understanding the funding process early. Requesting a care needs assessment, exploring financial support options, and reviewing care home choices carefully can make the transition into long-term care much easier to manage.
Planning ahead also helps caregivers make informed decisions about the cost of care homes, home care alternatives, and the best level of support for their loved one.
If you are supporting someone with dementia and need guidance navigating care home fees, funding assessments, or NHS Continuing Healthcare applications, Care Sync Experts can help.
We work with families and care professionals to review funding eligibility, explain the assessment process clearly, and help present care needs accurately so you can access the financial support available for dementia care and avoid the common mistakes that delay or reduce funding.
FAQ
Do dementia patients do better at home or in a nursing home?
It depends on the stage of dementia and the level of support the person needs. In the early stages, many people with dementia do well at home because familiar surroundings can reduce confusion and anxiety. Family support, home care services, and structured routines often help maintain independence for longer.
However, as dementia progresses, some individuals require 24-hour supervision, specialist dementia care, or nursing support. At this stage, a dementia care home or specialist nursing home may provide a safer environment with trained staff, structured activities, and secure facilities designed to support memory-related conditions. The best option depends on the person’s safety, medical needs, and the level of support available at home.
How fast can dementia progress?
Dementia progresses at different speeds depending on the type of dementia, the person’s age, and their overall health. Some people experience slow progression over many years, while others may decline more quickly.
On average, many people live between 4 and 10 years after diagnosis, although some individuals live much longer. Certain forms of dementia, such as vascular dementia, may progress in noticeable steps, while Alzheimer’s disease typically causes a gradual decline. Regular medical reviews, supportive care, and early intervention can sometimes help slow the impact of symptoms.
What are the signs dementia is getting worse?
As dementia progresses, symptoms usually become more noticeable and begin to affect daily life more significantly. Families often notice changes in memory, behaviour, and independence.
Common signs that dementia may be worsening include: – Increasing memory loss and confusion – Difficulty recognising familiar people or places – Problems with communication or finding words – Changes in behaviour or mood, such as agitation or anxiety – Difficulty managing everyday tasks like dressing, cooking, or taking medication – Greater need for supervision and personal care
When these signs appear, families may start considering additional support such as home care services or specialist dementia care.
What are four common behaviours that people with dementia often exhibit?
People living with dementia often experience changes in behaviour because the condition affects memory, reasoning, and emotional regulation. While symptoms vary from person to person, several behaviours commonly occur.
Four common behaviours seen in people with dementia include: Memory loss – forgetting recent events, appointments, or conversations Confusion or disorientation – becoming lost in familiar places or forgetting the date or time Mood or personality changes – increased anxiety, irritability, or withdrawal Repetitive actions or questions – asking the same question repeatedly or repeating activities
These behaviours usually develop gradually as the condition progresses. Understanding them can help caregivers respond with patience and choose the right level of support for the person living with dementia.
Are there new rules for care home payments introduced in 2026?
Care home fees in the UK continue to follow the existing means-tested system, with no lifetime cap on care costs and no automatic reduction in care home costs. Families must still plan based on income, savings, and property, as local authorities assess care home payments using the same framework that applied in previous years.
This guide explains what actually applies in 2026, clears up common myths, and shows how care home fees work in practice so families can make informed decisions.
Why So Many Families Expect New Care Home Rules in 2026
How to Get Referrals for Supported Living Without a Property | 2025 Framework Guide
Confusion around care home payments in 2026 did not come from nowhere. For several years, the government discussed major reforms to how care is funded in England. These plans received widespread media coverage and created the expectation that care home costs would become more predictable or capped.
Earlier proposals promised changes such as a lifetime cap on care costs and higher thresholds before people would need to pay for their own care. Many families assumed these reforms would eventually take effect, especially after repeated delays.
However, those proposals never became law. By 2026, the government had abandoned them entirely. Despite that, outdated information continues to circulate online, leading many people to believe the care home fees UK system has changed when it has not.
This mismatch between expectation and reality causes real problems. Families delay planning, underestimate care home costs, or assume protections exist that simply do not apply. Understanding what didn’t change in 2026 matters just as much as what did.
Were New Care Home Payment Rules Introduced in 2026?
No. No new care home payment rules have been introduced in 2026 (As of the time of publishing this content). Despite years of public discussion about reform, the legal framework for paying care home fees in the UK, particularly in England, remains the same.
Local authorities still use a means-tested system to decide who pays for care and how much they contribute. There is no lifetime cap on care costs, and there are no new protections that automatically reduce care home fees in 2026. Families should not assume that care home costs are capped, frozen, or subsidised simply because reforms were previously announced.
This point matters because many people plan care based on headlines rather than law. In practice, councils continue to assess:
A person’s income, such as pensions and benefits
Their capital, including savings and, in some cases, property
Whether they qualify for full, partial, or no local authority support
The absence of new rules also means responsibility has not shifted. Individuals with assets above the upper threshold still self-fund their care, while those below may receive council support. Nothing in 2026 changes how that assessment works.
It’s also important to be precise about geography. The care funding system discussed here applies primarily to England. Wales, Scotland, and Northern Ireland operate under different frameworks, with their own thresholds and rules. Many online articles blur this distinction, which adds to the confusion.
In short, 2026 did not bring reform, it brought continuity. Any decisions about paying for care home fees must still rely on the existing rules, not on plans that never took effect.
How Care Home Fees Work in the UK in 2026
Care home fees in the UK still work on a means-tested basis in 2026. Local authorities do not pay a flat rate, and they do not cover costs automatically. Instead, they assess each person’s financial situation to decide who pays, how much, and for how long.
When paying for care home fees, councils look at two things first: income and capital.
What Local Authorities Assess
During a financial assessment, the council considers:
Income, including state pensions, private pensions, and certain benefits
Capital, such as savings, investments, and, in some cases, property
If a person’s assets sit above the upper capital threshold, they must usually pay their own care home fees in full. If assets fall between the upper and lower thresholds, the council may contribute part of the cost, while the individual pays a means-tested amount. People with assets below the lower threshold receive the highest level of support, although they still contribute from their income.
This process applies whether someone enters a residential care home or a nursing home. It also explains why two people with similar care needs can face very different care home costs.
Why Care Home Fees Vary So Much
Care home fees UK families face differ widely because the system ties costs to personal finances, not just care needs. Location, type of care, and whether someone qualifies for council support all affect the final amount.
In many cases, families only realise how much care home fees can cost once assessments begin. That delay often leads to rushed decisions and unnecessary financial stress.
How Much Can You Keep Before Paying for Care in the UK?
Care Home Payments UK
How much you can keep before paying for care in the UK depends on your total capital, not just your income. In 2026, the financial thresholds used by local authorities in England remain unchanged, and they play a central role in deciding who pays care home fees.
Local councils assess capital using two key limits:
Upper capital limit: If your savings and assets exceed this level, you usually pay the full cost of your care.
Lower capital limit: If your assets fall below this level, the council provides the highest level of financial support, although you still contribute from your income.
If your capital sits between these two limits, the council applies a means-tested contribution. You pay what you can afford from your income, plus a tariff contribution based on your assets. This structure explains why people with similar savings can face very different care home costs depending on where their capital falls.
It’s important to understand that capital does not only mean money in the bank. Councils may also consider investments and, in some cases, the value of property. Misunderstanding what counts can lead families to assume they must self-fund when support may actually be available.
Because these thresholds determine whether care home costs come from personal funds or council support, knowing where you stand financially allows you to plan early and avoid unnecessary surprises.
What Counts as Capital When Paying for Care Home Fees?
When councils assess paying for care home fees, they look closely at a person’s capital, not just their income. Capital includes assets that someone could reasonably use to contribute toward their care home cost.
Assets That Usually Count as Capital
Local authorities typically include:
Savings held in bank or building society accounts
Cash and investments, such as ISAs, stocks, shares, and bonds
Premium Bonds and similar financial products
Property or land, if no qualifying exemption applies
These assets form the basis of how councils decide whether someone must self-fund or qualifies for support with care home fees UK families face in 2026.
Assets That Usually Do Not Count
Not everything a person owns counts as capital. Councils normally disregard:
Personal belongings, including furniture, jewellery, and vehicles
The value of a home, if a spouse, civil partner, or qualifying dependent continues to live there
Certain compensation payments or trust funds, depending on how they are structured
This distinction matters. Many families assume all assets count, which leads to unnecessary panic or rushed decisions.
Misunderstanding capital rules can increase care home costs unnecessarily. Some families believe they must sell assets immediately or that council support is unavailable, even when exemptions apply.
Capital assessments depend on individual circumstances, not assumptions. Before making decisions that affect long-term finances, families should understand exactly what councils include and exclude when calculating care home cost contributions.
Does Your Home Count Toward Care Home Costs?
In some cases, yes, your home can count toward care home costs, but it does not apply in every situation. How property is treated often makes the biggest difference to a family’s financial outcome, which is why misunderstandings here cause so much anxiety.
When someone moves permanently into a care home, the local authority may include the value of their home in the financial assessment. This usually happens if the property is empty and no qualifying person continues to live there. In that situation, the home becomes part of the capital used to calculate care home fees.
However, important exemptions apply, and many families overlook them.
When the Home Is Not Included
The council must disregard the value of a home if it remains occupied by:
A spouse or civil partner
A partner the person lives with
A dependent relative, such as a child under 18
In some cases, a close relative who is elderly or disabled
If any of these conditions apply, the home does not count toward care home costs, even if the person receiving care moves into a residential setting.
Temporary Disregards and Deferred Decisions
Even when a property does count, councils usually apply a temporary disregard period at the start of a care home placement. This gives families time to understand their options instead of making rushed decisions.
Many people assume selling the house is inevitable. In reality, councils often offer deferred payment arrangements, which allow care costs to be paid later from the property value rather than forcing an immediate sale.
Why Property Rules Matter So Much
Property often represents the largest single asset a person owns. Misunderstanding how it affects care home costs can lead families to sell too early or believe support is unavailable when it actually is.
Understanding when a home counts, and when it does not, creates space to plan properly and avoid unnecessary financial pressure.
How to Avoid Selling Your House to Pay for Care
Many families worry that moving into a care home automatically forces them to sell their house. In reality, selling your home is not always necessary, and the system offers lawful ways to manage care home costs without an immediate sale.
Use Property Disregards Where They Apply
If a spouse, partner, or qualifying dependent continues to live in the property, the council must ignore the home’s value during the financial assessment. In these cases, the house does not affect care home fees at all. Families should always confirm whether a mandatory disregard applies before considering any sale.
Ask About Deferred Payment Agreements
When no exemption applies and the property counts as capital, councils often offer a deferred payment agreement. This option allows the person receiving care to delay paying care home fees until the property is sold later, usually after death or when the home is eventually vacated.
With a deferred payment arrangement:
The council pays the care home fees upfront
The cost builds as a loan against the property
Families avoid selling the house under pressure
This approach gives families time and flexibility while ensuring care continues.
Avoid Rushed Decisions That Increase Costs
Some people try to transfer ownership of property or give away assets to avoid paying care home costs. Councils treat this as deliberate deprivation of assets and may still assess fees as if the property were owned.
Trying to bypass the rules often backfires and leads to higher long-term costs. Planning early and using recognised options protects both finances and peace of mind.
The best way to avoid selling a house to pay for care is understanding the rules before care becomes urgent. Early advice allows families to explore exemptions, payment arrangements, and alternatives without panic.
Are Next of Kin Responsible for Care Home Fees?
Financial Case for Live in Care 2026
In most situations, next of kin are not responsible for paying care home fees. Care costs remain the responsibility of the person receiving care, not their children, relatives, or family members.
This misunderstanding causes unnecessary fear. Simply being listed as next of kin does not create a legal duty to pay for care.
When Family Members Are Not Liable
You are not required to pay care home fees if:
You are a son, daughter, or relative with no legal agreement
You manage finances informally or help with paperwork
You act as an advocate or support person
Councils assess the care recipient’s finances only, not the family’s income or assets.
When Someone Might Become Responsible
A next of kin may become responsible for care home fees only if they:
Sign a contract or guarantee agreeing to cover costs
Choose a care home that charges more than the council’s rate and agree to pay a third-party top-up
Legally take on financial responsibility through a binding agreement
These situations involve choice, not obligation. No one should feel pressured to sign payment agreements without understanding the consequences.
Many families confuse emotional responsibility with legal responsibility. While relatives often help organise care, the law keeps financial liability separate unless someone actively agrees to take it on.
Understanding this distinction helps families plan care without unnecessary guilt or fear.
Do Dementia Sufferers Have to Pay Care Home Fees?
Yes, in many cases people with dementia do have to pay care home fees. A diagnosis of dementia on its own does not remove the requirement to contribute toward care home costs. The same financial assessment rules apply as they do for any other condition.
This often surprises families, especially when dementia leads to high and long-term care needs.
Why Dementia Does Not Automatically Remove Fees
Local authorities base care home fees on financial circumstances, not diagnosis. Even when someone lacks mental capacity or requires specialist dementia care, councils still assess income and capital in the same way.
That said, dementia can affect how care is funded, depending on the level and type of care required.
When NHS Funding May Apply
Some people with dementia qualify for NHS Continuing Healthcare, which covers the full cost of care, including accommodation. This funding depends on whether the person’s primary need is health-related rather than social care.
Eligibility does not depend on savings or property. Instead, it relies on a detailed assessment of care needs. Many families miss out because they assume dementia automatically qualifies someone for NHS funding, which is not the case.
The difference between local authority funding and NHS funding can be significant. Families should always request a proper assessment and challenge decisions where appropriate.
Understanding the distinction helps families avoid paying care home fees unnecessarily and ensures the right funding route applies.
How Much Do Care Homes Cost Per Week in the UK?
Care home costs in the UK vary widely, but in 2026 most families can expect to pay several hundred pounds per week, with prices rising significantly for nursing or specialist care.
On average:
Residential care homes often charge £700 to £1,000 per week
Nursing care homes commonly charge £900 to £1,400 per week or more
Specialist dementia care can exceed these ranges, depending on care intensity and location
These figures reflect national averages. Actual care home costs depend heavily on where the home is located, the level of care required, and whether local authority funding applies.
Why Weekly Care Home Costs Differ So Much
Care home fees UK families face are not fixed prices. Providers set fees based on:
Staffing levels and qualifications
Type of care (residential, nursing, dementia)
Property costs and facilities
Regional demand and local wage levels
Homes in London and the South East typically charge more than those in other regions. A basic residential placement may cost far less than a high-dependency nursing bed, even within the same area.
What These Numbers Mean for Planning
Weekly care home cost figures add up quickly over time. Without council support or NHS funding, long-term care can place significant pressure on savings and property.
This is why understanding funding rules, assessments, and alternatives matters before care becomes urgent.
Why Care Home Costs Vary So Widely
New Rules for Care Home Payments in 2026
Care home costs vary widely because no single factor determines pricing. Providers set fees based on a combination of care needs, location, staffing, and facilities, not just the length of stay.
Location Plays a Major Role
Geography strongly influences care home cost. Homes in areas with higher property prices and wages, such as London and the South East, usually charge more. In contrast, care homes in other regions often operate with lower overheads, which can reduce weekly fees.
Level and Type of Care Required
The type of care makes a significant difference. Residential care costs less than nursing care because nursing homes require registered nurses on site. Dementia care often costs more again, as it demands higher staffing ratios, specialist training, and enhanced safety measures.
Staffing and Quality Standards
Staffing represents one of the largest expenses for care homes. Homes that invest in experienced staff, continuous training, and higher staff-to-resident ratios often charge more. These costs reflect the level of care provided, not unnecessary mark-ups.
Facilities and Services
Modern facilities, private rooms, en-suite bathrooms, specialist equipment, and additional services all affect pricing. While these features do not change funding rules, they influence how care home costs compare between providers.
Why Comparing Prices Alone Can Mislead
Two care homes may charge very different fees while meeting the same regulatory standards. Comparing care home cost without considering care quality, staffing, and suitability often leads families to choose poorly.
Examples of Care Home Costs in Practice
Care home costs often make more sense when you see how they play out in real situations. While every provider sets its own fees, examples help show why prices differ and what families usually pay for.
Example 1: Residential Care in a Standard Setting
A care home similar in profile to Fairview Care Home may focus on residential support for older adults who need help with daily living but not constant medical care. In this type of setting, weekly costs often sit at the lower end of the national range.
Fees usually reflect:
Personal care and supervision
Meals and accommodation
Basic activities and social support
For many families, this level of care meets current needs without the higher costs associated with nursing or specialist services.
Example 2: Nursing or Dementia-Focused Care
A home comparable to Woodland Care Home may provide nursing care or specialist dementia support. These homes typically charge more because they operate with:
Registered nurses on site
Higher staffing ratios
Specialist dementia training and secure environments
Even within the same area, this type of care can cost several hundred pounds more per week than standard residential care.
What These Examples Show
These comparisons highlight an important point: care home costs reflect care complexity, not just accommodation. Two homes may appear similar from the outside but charge very different fees because they meet very different needs.
Families often focus on price alone, but choosing the wrong level of care can lead to additional moves, reassessments, and stress later on. Matching care needs to the right setting matters as much as managing cost.
Is Care Home Funding the Same as Home Care Funding?
Care home funding and home care funding follow similar principles, but they work very differently in practice. Understanding the difference helps families compare options realistically instead of assuming costs apply in the same way.
How Funding Assessments Compare
Both types of care usually involve:
A care needs assessment by the local authority
A financial assessment to determine contributions
In both cases, councils look at income and capital. However, how those assets affect costs changes depending on where care takes place.
The Key Difference: How Property Is Treated
The most important difference lies in property.
Care home funding:
When someone moves into a care home permanently, the value of their home may count toward care home fees unless an exemption applies.
Home care funding:
When someone receives care at home, the value of their property does not count at all. Councils exclude it because the person continues living there.
This distinction explains why some people who must self-fund a care home may still qualify for council support when receiving care at home.
Income Is Treated Differently Too
Income rules also differ:
People in care homes usually contribute most of their income toward fees, keeping only a small personal expenses allowance.
People receiving care at home retain more income to cover everyday living costs such as food, utilities, and housing.
Families often assume moving into a care home is the only option when care needs increase. In reality, home care can remain affordable for longer because funding rules are more flexible.
Comparing funding across care settings allows families to weigh cost, independence, and long-term sustainability rather than making decisions under pressure.
What Families Should Do Next When Planning Care in 2026
Planning care in 2026 requires clarity, not assumptions. Because the new rules for care home payments did not materialise, families must base decisions on the system that already exists.
Start by understanding the full picture:
Do not assume care home costs are capped. There is no lifetime cap on care costs in place.
Review finances early. Look at savings, income, and property before care becomes urgent.
Request proper assessments. A care needs assessment and a financial assessment determine support, not diagnosis alone.
Understand property rules. Know when a home counts toward care home fees and when exemptions apply.
Avoid rushed decisions. Selling property or signing payment agreements under pressure often leads to avoidable costs.
Ask about alternatives. Home care or deferred payment arrangements may reduce immediate financial strain.
Seek regulated advice. Complex cases benefit from professional guidance before long-term commitments are made.
Families who plan early have more options. They avoid unnecessary sales, challenge incorrect assumptions, and make choices that fit both care needs and financial reality.
Care funding remains one of the most complex parts of the UK care system. Understanding how it actually works in 2026 gives families the confidence to act, rather than react.
Care Home Payments in 2026: Key Points at a Glance
No new rules for care home payments were introduced in 2026.
Care home fees in the UK continue to follow a means-tested system.
There is no lifetime cap on care costs in place.
Local authorities assess income, savings, and, in some cases, property.
People with assets above the upper threshold usually self-fund their care.
A person’s home may count toward care home costs, unless an exemption applies.
Next of kin are not automatically responsible for paying care home fees.
Dementia does not remove the requirement to pay care home fees, although NHS funding may apply in some cases.
Care home costs vary widely based on location, care type, and care needs.
Need clarity on care home funding decisions in 2026?
Paying for care often becomes urgent before families fully understand the rules. Confusion around care home fees, property assessments, and funding thresholds can lead to rushed choices that increase long-term costs.
Care Sync Experts helps families and care providers across England, Wales, and Northern Ireland understand how care funding works in practice, before financial pressure forces difficult decisions. Support typically includes:
Clear explanations of care home funding rules and assessments
Guidance on property treatment, exemptions, and deferred payment options
Support understanding eligibility for local authority or NHS funding
Practical planning to avoid unnecessary asset loss
Independent, regulation-aligned advice grounded in current UK guidance
If you’re unsure how care home costs will be assessed, whether property will be included, or what options exist before committing to long-term care, a short conversation now can prevent avoidable stress later.
This article reflects UK care funding rules and sector practice as at 2026. Funding decisions depend on individual circumstances and may change. Families should always refer to current guidance from the relevant local authority or regulator.
FAQ
Can the government take your house to pay for care in the UK?
The government does not usually “take” your house outright. If you move permanently into a care home, the local authority may include your home’s value in the financial assessment if no qualifying person still lives there.
If you qualify for a deferred payment agreement, the council can pay fees upfront and recover the money later from your estate, often by placing a legal charge against the property rather than forcing an immediate sale.
What happens when money runs out for care home UK?
If someone self-funds and their savings fall below the upper threshold, they should contact the local authority early and request a financial assessment.
From that point, the council may begin contributing to care costs, but it may not pay the full care home fee, especially if the home charges more than the council’s usual rate. In that situation, the person may need to:
– move to a home within the council’s budget, – or arrange a third-party top-up (someone else pays the difference), if available.
Planning ahead matters because delays can create arrears and reduce options.
How much does a caare home cost per month in the UK?
A monthly estimate depends on the weekly fee. Many care homes charge hundreds to over a thousand pounds per week, so monthly costs commonly land in the low-to-mid thousands.
A simple way to estimate: Weekly fee × 52 ÷ 12 = monthly cost Example: £900/week → £900 × 52 = £46,800/year → ÷ 12 ≈ £3,900/month
This varies by region, care type (residential vs nursing), and whether specialist dementia support is needed.
What is the 7 year rule for care home fees in England?
There is no fixed “7-year rule” that guarantees protection from care fee assessments. People often confuse care fee rules with inheritance tax gifting rules.
In England, councils look at whether someone deliberately reduced assets to avoid care charges (often called deprivation of assets).
If the council decides a person gave away money or property to reduce care costs, it may still treat them as if they still own those assets, regardless of how long ago the transfer happened.
Because this area is fact-specific, families should get proper guidance before making major transfers.
Starting a care home in the UK means registering with the Care Quality Commission (CQC) before you provide any residential care for adults in England.
To open a care home, you must register the provider (and usually a registered manager), define the regulated activities you’ll deliver, prove you can meet quality and safety standards, and prepare for inspection.
Most delays happen because owners secure property or hire staff before they design the service around CQC expectations, so start with compliance, then build everything else around it.
How to start a care home: pick your care model first
How to Set Up a Care Agency – Everything You Need to Know for 2025
Before you apply to CQC or spend money on property, decide what kind of care home you’re actually opening. This single decision shapes your registration route, staffing, costs, and long-term risk.
Residential care homes (most common starting point)
Residential care homes support adults who need help with daily living, washing, dressing, eating, mobility, and medication prompts, but not 24-hour nursing care.
If this is your first time starting a care home, this model usually makes sense because:
Registration is more straightforward
Staffing requirements are lower than nursing homes
Startup and operating costs are easier to control
Demand is strong in most local authority areas
Many first-time owners choose residential care, build a strong compliance record, then expand later.
Nursing homes (higher risk, higher complexity)
Nursing homes provide everything a residential home does plus continuous nursing care. You’ll need registered nurses on duty, more complex clinical governance, and higher insurance cover.
Choose this route only if:
You already have nursing leadership in place, or
You’re converting or acquiring an existing nursing home, or
You’ve secured funding that supports higher staffing and clinical costs
If you underestimate the clinical side, inspectors will spot it quickly.
Specialist care homes (dementia, learning disability, mental health)
Specialist homes focus on a specific need, such as dementia or learning disabilities. These services attract strong demand, but inspectors expect evidence of specialist training, adapted environments, and tailored care models from day one.
Specialism works best when:
You have direct experience with the client group
Your location already has referral pathways
Your staffing plan reflects the higher support needs
Respite care homes (short-stay focus)
Respite care provides short-term placements for people whose usual carers need a break or who are transitioning from hospital. While stays are shorter, standards are not lighter. You still need full compliance, safe staffing, and strong admission controls.
A simple decision rule
If you’re unsure how to start a care home, use this rule:
Start with the least complex care model you can run safely, then scale once you’ve passed inspections and stabilised occupancy.
CQC does not reward ambition. It rewards clarity, safety, and control.
How to open a care home in England: what CQC expects
2026 Guide to Starting Home Care
If you want to open a care home in England, you must register with the Care Quality Commission (CQC) before you provide any regulated care. You cannot trade first and “sort registration later.” Doing so is a criminal offence and will end your application before it starts.
You register the provider, and usually the manager too
CQC does not register buildings. It registers people and organisations.
If the provider is an organisation or partnership, CQC will also expect you to appoint and register a registered manager who takes day-to-day responsibility for the service.
If you apply as an individual and intend to manage the home full time yourself, you may not need a separate manager, but CQC will still assess you against the same standards.
The key question inspectors ask is simple: Who is legally accountable for safe, well-led care every day?
What you submit with your CQC application (plain English)
CQC applications fail when owners treat them like paperwork. In reality, this is where you prove you understand the business you’re starting.
You must clearly set out:
Each location where you will deliver residential care
The regulated activities you intend to carry out
Who your service is for and who it is not for
How you will meet quality and safety standards
A formal declaration of compliance
CQC will also assess:
Your governance structure
Your ability to recruit, train, and supervise staff
Your financial viability
Your understanding of safeguarding, medicines, and risk management
There is no application fee, but once CQC grants registration, you must pay an annual fee to remain registered.
A critical warning (where most people go wrong)
Many first-time owners secure property, buy equipment, or hire staff before they fully understand what CQC expects. That approach increases cost and risk.
A safer rule when starting a care home in the UK is this: Design the service on paper first, prove it meets CQC standards, then commit money.
CQC approves services that show control, clarity, and realistic planning, not enthusiasm alone.
What inspectors actually look for (so you build the right service)
How To Start a Homecare Business
When CQC assesses your application and later inspects your care home, inspectors don’t look for perfection. They look for control. They want clear evidence that you understand your risks and manage them every day.
Staffing: enough people, with the right skills
There is no legal staff-to-resident ratio for care homes. Instead, inspectors judge whether you provide sufficient, competent staff to meet residents’ needs at all times.
In practice, this means you must be able to show:
How many staff you need on each shift
Why that number works for your residents’ needs
How you cover sickness, holidays, and emergencies
How staff receive training, supervision, and support
If you can’t explain your staffing logic clearly, inspectors will assume it isn’t safe.
Safeguarding and risk management
Inspectors expect safeguarding to run through everything you do, not sit in a policy folder.
They will look for:
Clear safeguarding procedures that staff actually understand
Risk assessments tailored to individual residents
Evidence that staff know how to raise concerns and act quickly
Good providers don’t just react to incidents. They anticipate risk and reduce it early.
The same standard applies to care records. Inspectors expect notes that are clear, current, and reflect real care, not copy-and-paste templates.
Leadership and governance
CQC places heavy weight on whether a service is well-led. Inspectors want to see:
Clear responsibility at management level
Regular audits and checks
Evidence that you learn from mistakes
Systems that improve care over time
This applies even to small homes. Size does not reduce accountability.
The inspection mindset you need
If you’re starting up a care home, adopt this mindset early: If you can’t evidence it clearly, you can’t defend it.
Strong services don’t rely on goodwill or hard work alone. They rely on systems that work even on bad days.
Starting a care home UK, a practical setup checklist
Once you understand the care model and CQC expectations, you can move into setup. The order matters. Follow these steps to avoid wasted money, failed applications, and long delays.
1) Confirm demand and referral routes
Start with evidence, not assumptions.
Check local authority commissioning priorities
Identify who will refer residents (councils, hospitals, families)
Define the exact needs you will accept, and those you won’t
Clear admission criteria protect residents and your registration.
2) Secure a suitable property (with safety in mind)
Choose a building that can realistically meet care standards.
Adequate space for mobility aids and equipment
Safe access and evacuation routes
Fire safety suitability from day one
Avoid heavy renovations until your service model and compliance plan are clear.
3) Build your compliance pack before hiring
Create the core documents that prove control:
Safeguarding procedures
Medicines management
Staffing and supervision plans
Risk assessments
Governance and audit processes
Inspectors expect these systems to exist before residents arrive.
4) Appoint or identify your registered manager
CQC places major responsibility on leadership.
Confirm who holds day-to-day accountability
Align their experience with your care model
Prepare their registration alongside the provider application if required
Weak leadership delays or blocks registration.
5) Plan staffing and training realistically
Design rotas around resident needs, not minimum numbers.
Cover nights, weekends, sickness, and leave
Schedule induction and mandatory training
Build supervision and appraisal into normal operations
Staffing failures cause most early enforcement action.
6) Apply to CQC with a complete, coherent application
Submit only when everything aligns:
Service description
Regulated activities
Locations
Governance systems
Financial viability
Rushed or inconsistent applications trigger long follow-ups.
7) Prepare for inspection before it happens
Assume inspectors will arrive.
Run internal checks
Test procedures with staff
Fix gaps early
The strongest providers treat inspection readiness as normal operations, not a one-off event.
Starting a care home, costs, funding, and cashflow reality
Starting a care home in UK
Starting a care home is capital-intensive, and most first-time owners underestimate how long it takes before income stabilises. If you plan costs realistically from the start, you protect the service and your registration.
The main cost areas to plan for
While figures vary by location and size, costs usually fall into these buckets:
Property
Purchasing or leasing a suitable building is often the largest upfront cost. Prices vary widely by region, and not every building can meet care standards without expensive adaptations.
Staffing (your biggest ongoing expense)
Wages typically account for the largest share of monthly outgoings. This includes care staff, management, training time, sickness cover, National Insurance, and pension contributions.
Compliance and governance
Training, audits, record-keeping systems, insurance, and ongoing quality monitoring all carry costs. These aren’t optional extras, they’re core operational expenses.
Equipment and environment
Beds, hoists, mobility aids, specialist seating, bathroom adaptations, and safety equipment add up quickly. Buying the right equipment early reduces injury risk and staffing strain.
Operating costs
Utilities, food, cleaning supplies, maintenance, professional fees, and marketing all need to sit within a realistic monthly budget.
Funding options to consider
Most people starting up a care home combine several funding sources:
Commercial mortgages for the property
Personal or investor capital
Business loans or asset finance for equipment
In some cases, targeted grants linked to specialist care or innovation
Lenders and investors will expect a clear business plan, realistic occupancy assumptions, and evidence that you understand regulatory risk.
The cashflow rule that protects new services
Even well-planned care homes take time to reach stable occupancy. A safe rule is this: Plan enough working capital to run the home for several months with low occupancy.
This buffer gives you room to:
Pass inspections without panic
Recruit and train staff properly
Build referrals without cutting corners
Care homes don’t fail because demand disappears. They fail when cashflow collapses before systems mature.
Business plan for a care home, what actually matters
A care home business plan is not a formality. Regulators, lenders, and partners use it to judge whether you understand the risks of starting a care home and whether your service can survive pressure.
Keep it practical. Avoid generic business language.
Executive summary (short, factual, focused)
State clearly:
What type of care home you’re opening
Where it will operate
Who it will serve
How it will stay safe, compliant, and financially viable
This section should make sense on its own.
Service model and staffing plan
Explain:
Your care model (residential, nursing, specialist, or respite)
Admission criteria and exclusions
Staffing structure by shift
How you recruit, train, and retain staff
Decision-makers want to see that staffing levels match resident needs, not optimistic assumptions.
Compliance and governance plan
Show how you will meet regulatory expectations daily:
Inspectors and lenders look for realism, not ambition.
Risk management
Identify the risks most likely to damage the service:
Staffing shortages
Inspection failure
Low occupancy
Rising costs
Then explain how you reduce and manage them.
A final business-plan rule
If your business plan can’t explain how the care home stays safe on a bad week, it isn’t finished.
How to set up a care agency instead (domiciliary care)
Many people who search for how to start a care home later realise that a residential setting isn’t the right first step. If you want lower startup costs and more flexibility, setting up a care agency (domiciliary care) may be a better option.
This model lets you deliver care in people’s homes rather than running a fixed premises.
How do I start a care agency?
If you’re asking how do I start a care agency, the process still begins with regulation, but the structure is different.
In England, you must register with the Care Quality Commission to provide personal care in people’s homes. As with care homes, you register the provider, and usually a registered manager, before delivering any care.
The key difference is scale:
No residential property to buy
Lower equipment costs
Staffing flexibility based on demand
However, compliance expectations remain just as strict.
How to start a care agency UK: what changes
When learning how to start a care agency UK, focus on these areas early:
Recruitment and retention of carers
Scheduling and travel time management
Lone-worker safety
Accurate care records across multiple locations
Strong supervision and spot-check systems
Domiciliary care agencies often fail because growth outpaces control. Inspectors look closely at how you monitor care delivered off-site.
Domiciliary care agency business plan: what to include
A strong domiciliary care agency business plan differs from a care home plan in a few key ways:
Cashflow depends on care hours delivered, so accuracy matters.
Running a care agency: what breaks first
When running a care agency, problems usually appear in three places:
Missed or late visits due to poor rota planning
Inadequate supervision of carers working alone
Inconsistent care records that don’t reflect real visits
Strong agencies fix these early with:
Digital scheduling
Regular supervision
Clear escalation procedures
Care home vs care agency: a quick decision rule
If you want faster setup and lower risk, a care agency often makes sense first. If you want long-term asset value and can manage higher costs, a care home may suit you better.
Choose the model you can control safely, not the one that sounds more impressive.
Conclusion
Starting a care home in the UK is beyond a business decision, it’s a long-term responsibility. The providers that succeed don’t rush the process or rely on assumptions. They choose the right care model, design their service around regulatory expectations, control risk early, and build systems that hold up under inspection, commissioning scrutiny, and growth.
Whether you’re opening a residential care home or deciding that a domiciliary care agency is the better first step, the same principle applies: compliance comes first, sustainability comes next, and growth follows good governance, not the other way around.
Need expert support to strengthen your care service’s readiness?
Running a care service means operating under constant scrutiny. Even providers delivering good care can struggle with unclear accountability, documentation that doesn’t match day-to-day practice, or expansion that outpaces governance.
Care Sync Experts supports care homes and domiciliary care agencies across England, Wales, and Northern Ireland to build strong foundations before problems escalate. Support typically covers:
If you’re unsure whether your systems would stand up to inspection, commissioning review, or planned expansion, a short conversation now can prevent costly disruption later.
This article reflects UK care regulation and sector practice as at 2026. Requirements may change, and providers should always refer to current guidance from the relevant regulator.
FAQ
Is a care home business profitable in the UK?
A care home can be profitable, but margins depend on occupancy, staffing control, and funding mix. Well-run homes with stable occupancy often achieve single-digit to low-teens net margins, not the high margins people assume.
Profitability improves when the home maintains consistent referrals, controls agency staffing costs, and avoids compliance failures that trigger enforcement or closures. Poor management, not lack of demand, is the main reason care homes struggle financially.
How much does a care home cost in the UK?
The cost of starting a care home in the UK varies widely. Property alone can range from hundreds of thousands to several million pounds, depending on size and location.
Beyond the building, owners must budget for staffing, equipment, compliance systems, insurance, and working capital to cover low occupancy in the early months. Most failures happen when owners underestimate cashflow needs, not the headline purchase price.
How do care agencies get clients in the UK?
Care agencies typically get clients through local authority commissioning, NHS referrals, private self-funding clients, and word-of-mouth. Many councils use frameworks or Dynamic Purchasing Systems (DPS), meaning agencies must apply and meet quality thresholds before receiving referrals.
Private clients often come through online visibility, hospital discharge teams, and community networks. Agencies that combine public contracts with private clients tend to be more stable.
How much do care agencies charge per hour in the UK?
Hourly rates for home care agencies in the UK vary by region and funding source. Local authority rates are usually lower, while private client rates are higher to reflect travel time, staffing costs, and compliance overheads.
Rates also depend on the level of care required, time of day, and visit length. Agencies that price too low often struggle to retain staff and maintain quality, which quickly leads to regulatory issues.