A CQC Statement of Purpose is a legally required document that explains what your care service does, where it operates, and who it supports. If you provide a regulated activity in England, you must submit a clear, accurate Statement of Purpose as part of your CQC registration and keep it up to date as your service changes.
For a domiciliary care or supported living provider, this document does more than support an application. It defines the real scope of your service. It should show the Care Quality Commission exactly which regulated activities you provide, the people you intend to support, the locations you manage from and the leadership arrangements behind your care delivery.
A strong Statement of Purpose helps you avoid a common registration mistake: promising services that your staffing, training, policies or governance systems cannot yet support. It should match the care you plan to deliver every day, not read like a marketing brochure.
In this guide, we explain what a CQC Statement of Purpose must include, how to write it for domiciliary care and supported living, and how to make sure it aligns with your wider CQC registration documents.
What Is a CQC Statement of Purpose?
A CQC Statement of Purpose is a formal document that tells the Care Quality Commission what your service is set up to provide. It explains your care business in practical terms: the regulated activities you deliver, the people you support, the places you operate from and the managers responsible for day-to-day delivery.
For care providers, this document acts as a clear operating boundary. It helps you define what your team can safely provide now, rather than what you may hope to offer in the future.
For example, a domiciliary care provider may state that it delivers personal care to adults aged 18 and over in their own homes across a defined local area. A supported living provider may explain that it supports adults with learning disabilities, autism or mental health needs within specific supported living settings.
The Statement of Purpose should reflect your real service model. That means it should match your staffing arrangements, care policies, training plans, safeguarding processes, care assessments and business plan.
The role of the Care Quality Commission is to regulate health and adult social care services in England and check whether providers meet the care quality standards expected of registered services. Your Statement of Purpose helps CQC understand what it should expect from your organisation during registration, monitoring and inspection.
It also gives service users, families and professionals a clear picture of what your service offers. That is why you should write it in plain, factual language and avoid vague promises such as “we provide excellent care for everyone.” Instead, explain exactly who you support, what care you provide and how your team delivers it safely.
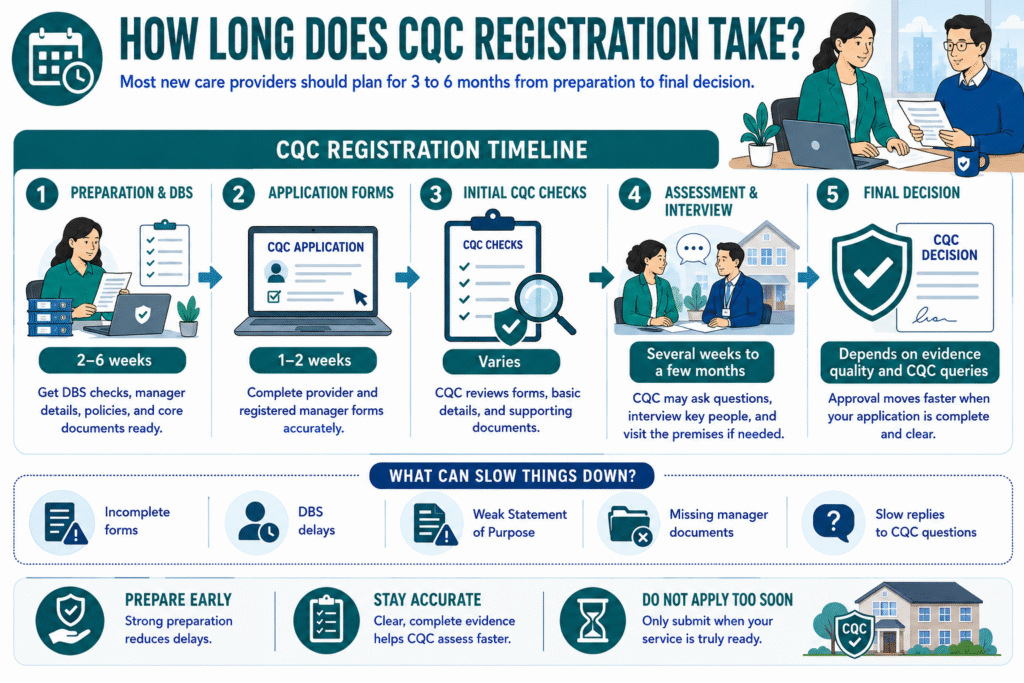
RELATED: How Long Does CQC Registration Take? 2026 Update
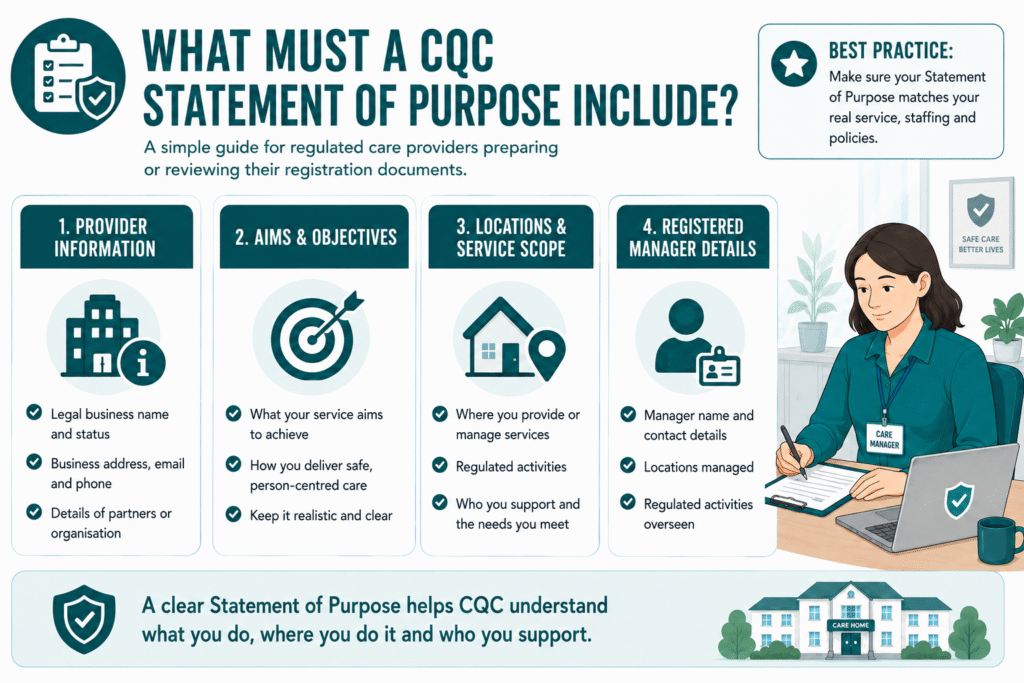
What Must a CQC Statement of Purpose Include?
Your CQC Statement of Purpose must give a clear, factual picture of your care business. It should explain what you provide, who you support, where you operate, and who manages the service.
Use the table below as a practical guide when preparing your document.
| Required area | What you should include | Practical provider tip |
| Provider information | Your legal business name, legal status, business address, telephone number, email address and details of any partners | Make sure these details match your registration forms, insurance documents, Companies House records and website |
| Aims and objectives | What your service aims to achieve and how you plan to deliver care | Keep this realistic. Do not promise services, response times or specialist support that you cannot yet evidence |
| Regulated activities | The exact regulated activities you are applying to provide | Use the same wording across your CQC application, Statement of Purpose and supporting documents |
| People you support | The age groups, needs and service-user bands your care business supports | Be specific. For example, state whether you support adults with dementia, physical disabilities, learning disabilities or mental health needs |
| Locations and service areas | Each location you operate from, contact details, service type and geographical area covered | For domiciliary care, explain where your office is based and the areas where your care workers provide support |
| Registered manager details | The registered manager’s name, contact details, locations managed and regulated activities they oversee | Check that manager details match the information included in their CQC application or registration records |
A good CQC Statement of Purpose does not try to impress with broad claims. It gives CQC a clear and accurate description of your service.
For example, rather than saying:
“We provide exceptional care to all people in the community.”
You could write:
“We provide personal care to adults aged 18 and over in their own homes across [local area]. We support people with physical disabilities, dementia and long-term health conditions, subject to individual assessment, staff competence and safe care planning.”
That level of detail helps CQC understand your service scope and helps your team stay clear about what your care business is responsible for delivering.
READ MORE: NHS Capacity Tracker: What Care Providers Need to Know in 2026
Write Your Scope Like a Care Provider, Not a Marketing Team
Your Statement of Purpose should describe the care you can deliver safely today. It should not read like a sales page or promise every type of support a family may ask for.
From a caregiver business standpoint, your scope affects staffing, training, care planning, risk management, and referrals. When you describe your service clearly, your care team knows who you can support and when you may need to seek specialist input or decline a referral.
Before you write this section, ask:
- Who do we support?
- What age groups do we accept?
- Which care needs can our staff safely manage?
- Which regulated activities do we provide?
- Where do we deliver care?
- What support do we not currently provide?
- When do we refer or escalate to another professional or service?
For a CQC Statement of Purpose domiciliary care service, you may explain that you provide personal care in people’s homes within a defined area. You may also state whether you support people with dementia, mobility needs, learning disabilities or long-term conditions.
For a CQC Statement of Purpose supported living service, you should explain the type of support offered, the people you support, the locations involved and the boundaries between regulated personal care and housing-related support.
Avoid vague wording such as:
“We provide outstanding care to everyone in the community.”
Use clear wording instead:
“We provide personal care to adults aged 18 and over in their own homes across [area]. We support people with dementia, physical disabilities and long-term health conditions where we can meet their assessed needs safely through trained staff, individual care plans and appropriate management oversight.”
Your scope should also match your CQC policies and procedures for domiciliary care, staff training, safeguarding arrangements and care planning process. If you say you provide complex care, 24-hour support or specialist dementia care, you should be able to show how your team will deliver it safely and consistently.
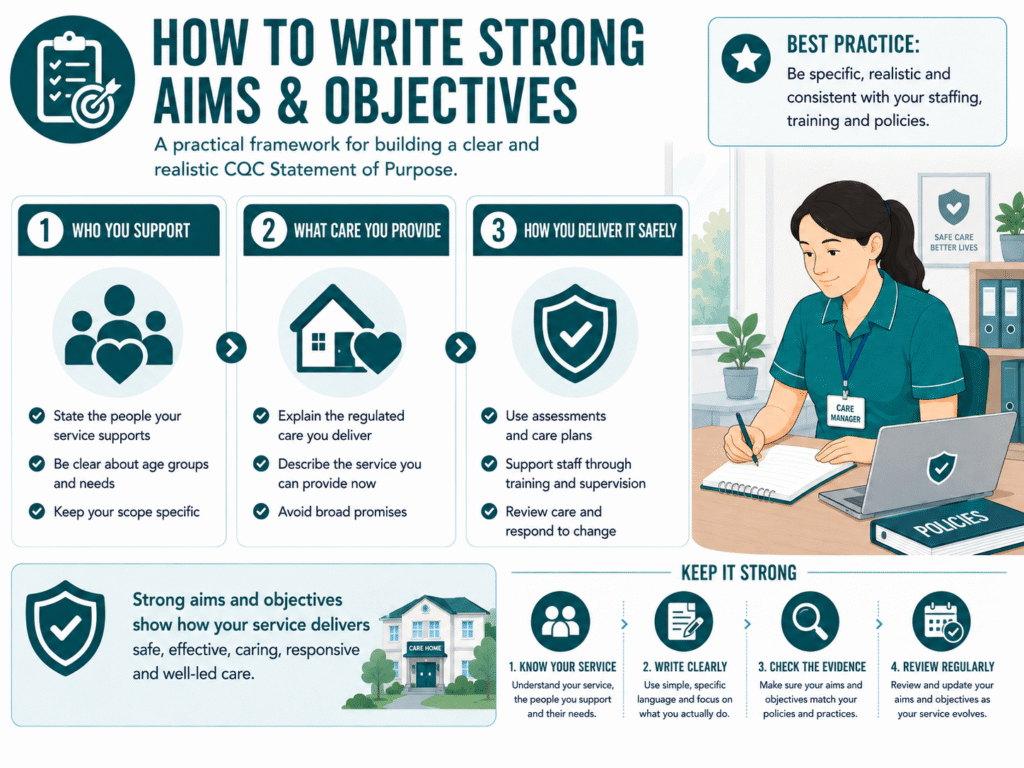
How to Write Strong Aims and Objectives
Your aims and objectives explain what your care service wants to achieve and how your team will deliver care in practice. They should show your values, but they also need to stay realistic, measurable and consistent with your staffing, training and governance systems.
A simple way to write them is to cover three points:
- Who you support
State the people your service is designed to support. - What care you provide
Explain the type of care, support or regulated activity you deliver. - How you deliver it safely and respectfully
Describe the practical systems behind your service, such as assessments, care plans, reviews, communication, supervision and training.
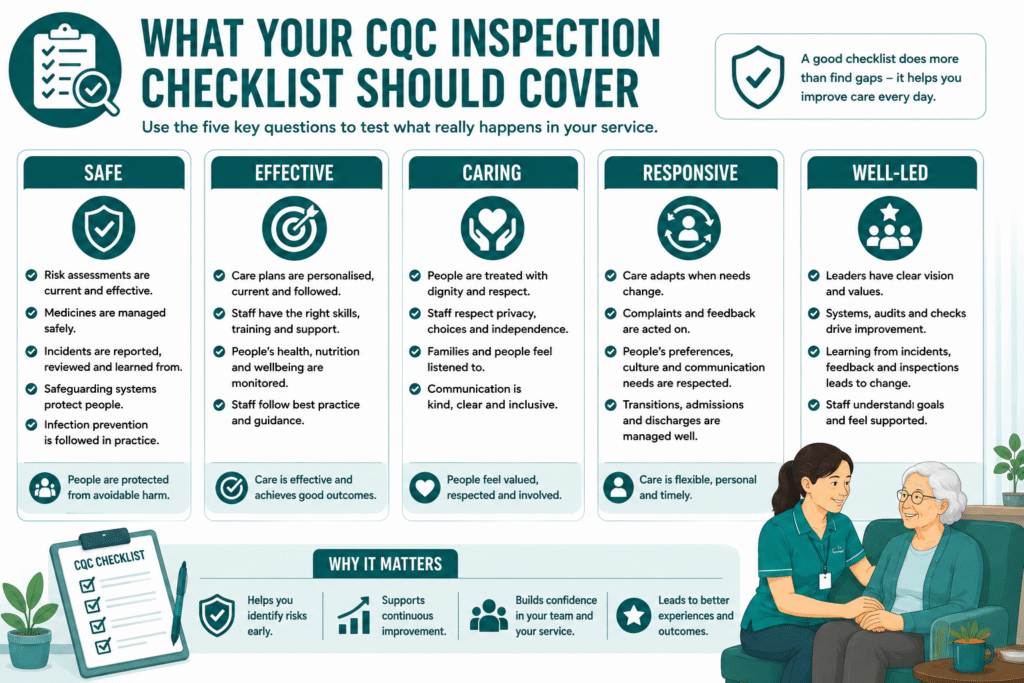
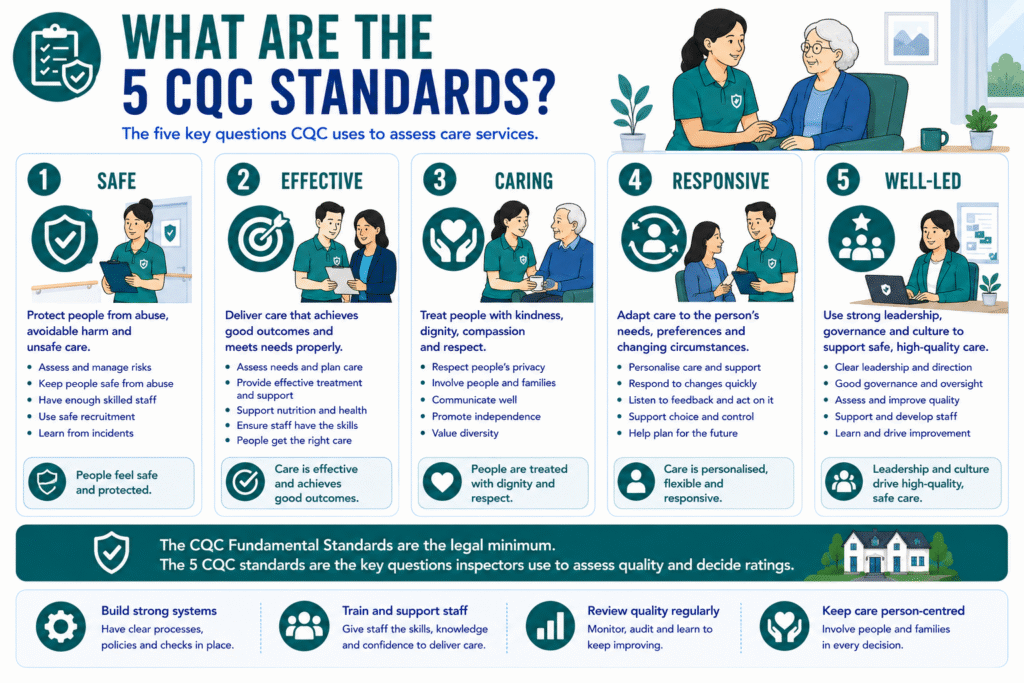
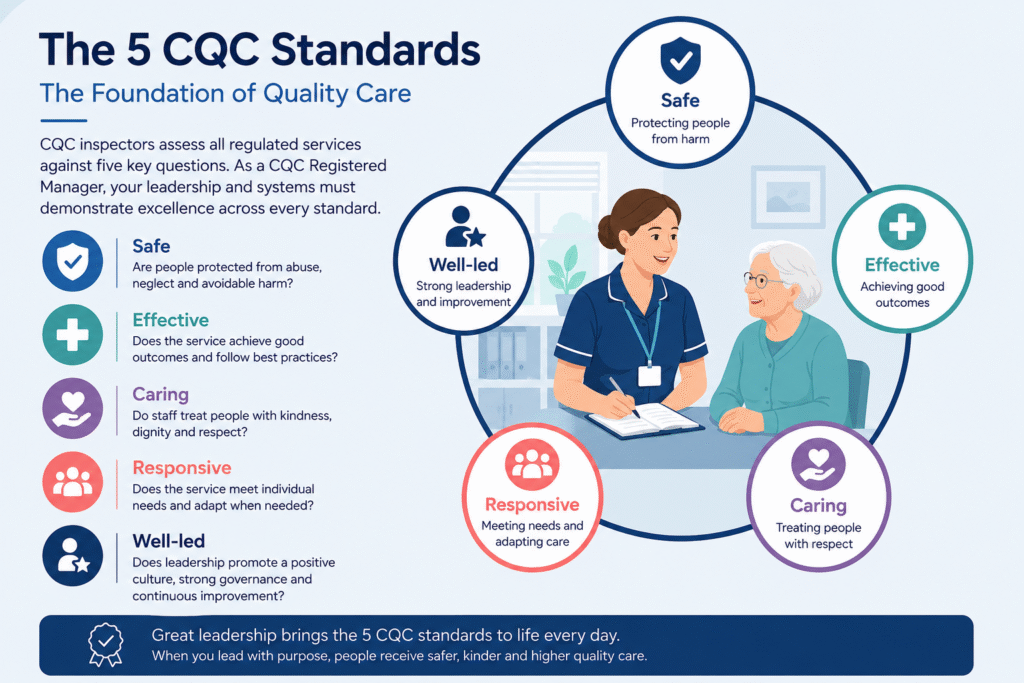
Your wording should reflect the CQC fundamental standards and the five key questions CQC uses when assessing services: safe, effective, caring, responsive and well-led. These are often what people mean when they search for “what are the 5 CQC standards.”
Here is an example for a domiciliary care provider:
“[Agency name] aims to provide safe, person-centred personal care to adults in their own homes across [area]. We support people to maintain independence, dignity and choice through care plans built around their assessed needs, preferences and routines.
We review care regularly, respond to changes in need, work with families and professionals where appropriate, and keep clear records to support safe decision-making. We recruit suitable care workers and support them through induction, supervision, CQC training and ongoing development.”
Strong aims and objectives should sound like something your team can genuinely deliver. Avoid promises such as “we will provide the highest standard of care at all times” unless you explain what that looks like in everyday practice.
The best statements give CQC, care workers and families a clear answer to one question: what will this service do, and how will it do it well?
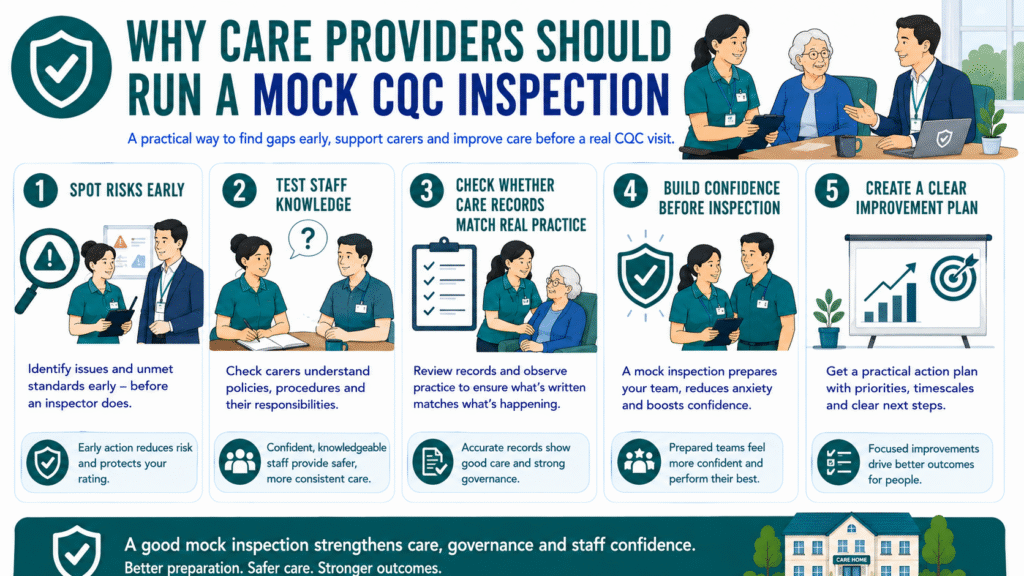
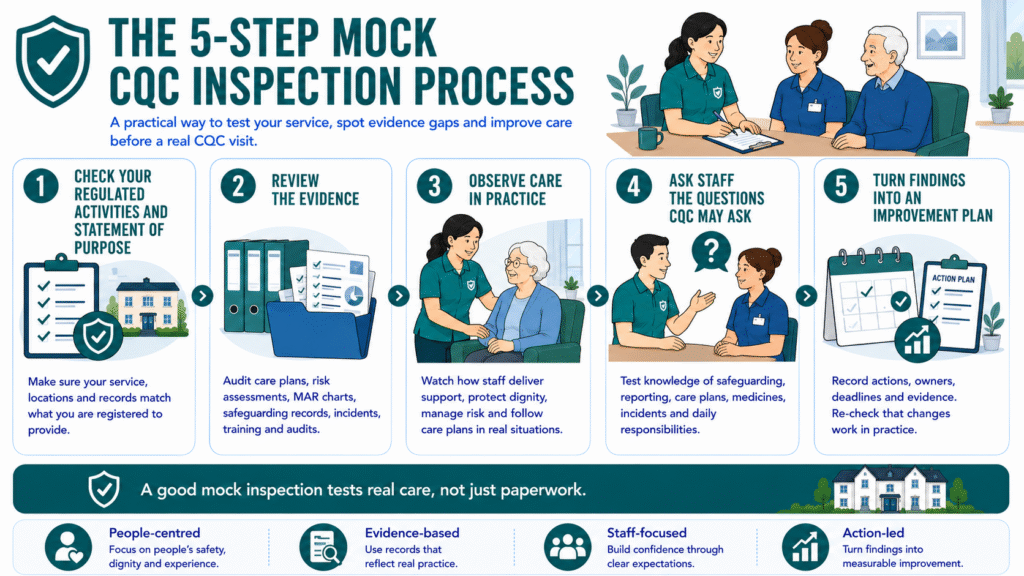
SEE ALSO: Mock CQC Inspection: A Practical 2026 Checklist for Care Providers
Make Sure Your Statement Matches Your Day-to-Day Care Service
Your Statement of Purpose should match how your care business actually operates. CQC may compare it with your registration documents, policies, staffing arrangements and the evidence you use to manage quality.
For a domiciliary care provider, this means checking that your Statement of Purpose aligns with:
- Your business plan and service-user guide
- Your staffing structure and on-call arrangements
- Your recruitment, induction and supervision process
- Your care assessments, risk assessments and care plans
- Your safeguarding, complaints and medication policies
- Your CQC policies and procedures for domiciliary care
- Your website, brochures and referral information
- Your training matrix and competency checks
This matters because your wording creates expectations. If you state that you provide dementia care, complex care, 24-hour support or specialist support for people with learning disabilities, your team must have the right skills, training, policies and management oversight to deliver that service safely.
Your Statement of Purpose does not replace your CQC training plan. However, it should reflect the level of care your staff can provide. For example, if your service supports people with medication needs, your care workers need suitable medication training, competency checks and clear escalation procedures.
The same principle applies to supported living. Do not describe regulated personal care unless you hold, or are applying for, the correct regulated activity and can show how staff will deliver that care safely.
A clear Statement of Purpose protects your care business. It helps your team understand service boundaries, supports safer referrals and reduces the risk of promising support that your current systems cannot safely provide.
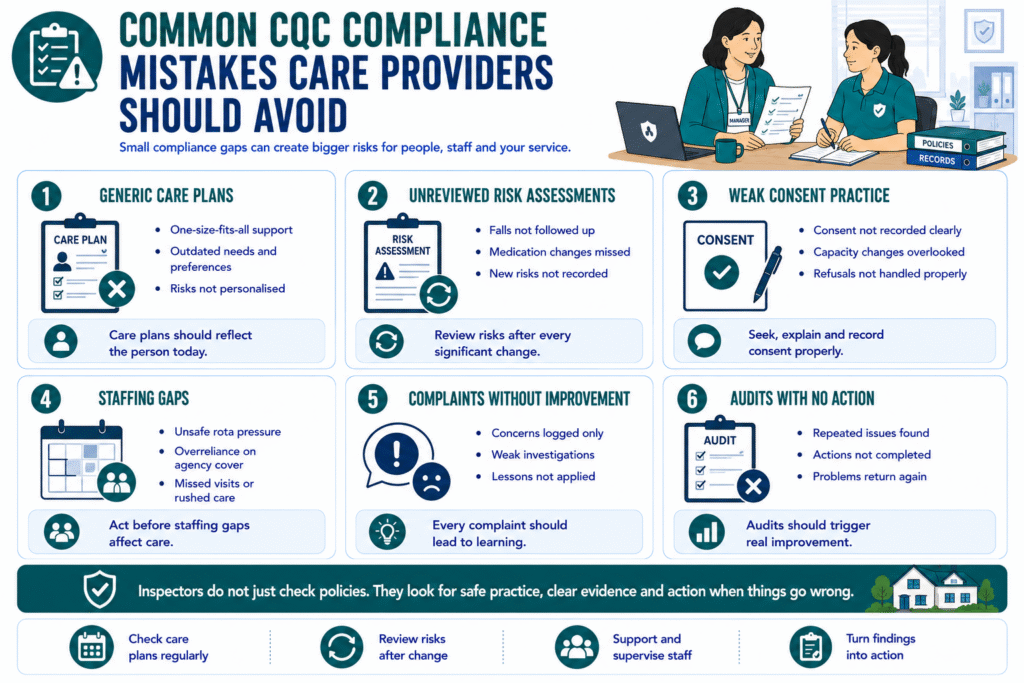
Common CQC Statement of Purpose Mistakes
Many providers lose time during registration because their Statement of Purpose sounds polished but does not clearly explain how the service will operate.
Avoid these common mistakes:
- Copying a generic statement of purpose template without tailoring it to your care business.
- Listing services you cannot safely deliver yet, such as complex care, 24-hour support or specialist dementia care.
- Using vague service-user descriptions, such as “all adults” or “everyone in the community.”
- Giving unclear location details or failing to explain where care takes place.
- Using different information across documents, such as one service area on your website and another in your registration paperwork.
- Writing broad aims without practical detail, for example promising “excellent care” without explaining care planning, reviews, staffing or communication.
- Forgetting to update the document after changing your manager, contact details, regulated activities, service-user groups or service model.
- Treating the Statement of Purpose as a one-off form instead of a live governance document.
A stronger approach is to review your Statement of Purpose whenever your care business changes. Ask whether your staff, training, policies and care systems still match what the document says you provide.
For example, if you begin supporting people with more complex needs, do not simply update your marketing. First check that your risk assessments, staff competence, medication processes, supervision arrangements and escalation pathways support that change safely.
A clear and accurate Statement of Purpose gives CQC a reliable picture of your service. It also helps care workers understand the limits of their role and gives families confidence about the type of support they can expect.
MORE: What Are the CQC Fundamental Standards? 2026 Update
When Should You Update Your Statement of Purpose?
You should review your Statement of Purpose whenever your service changes. It must remain accurate, because it tells CQC, service users and families what your care business provides.
Common reasons to update it include:
- You change your business address, phone number or email address.
- You appoint a new registered manager.
- You open, close or move a location.
- You change your service area.
- You begin supporting a different age group or new care needs.
- You add or remove a regulated activity.
- You change how your service delivers care.
- You expand into supported living, live-in care, complex care or another specialist area.
For example, a domiciliary care provider may start by supporting older adults with personal care in one local area. If the provider later begins supporting younger adults with learning disabilities or expands into another region, the Statement of Purpose should reflect that change.
Do not wait until an inspection to discover that your documents no longer match your service. Update the document as soon as the change is confirmed, then make sure your policies, staffing, training and public information reflect the same position.
Some changes may require more than an updated Statement of Purpose. If you want to add a new regulated activity, change a location or make another material registration change, you may also need to submit the correct notification or variation request to CQC.
Treat your Statement of Purpose as part of your ongoing governance. Review it regularly, keep a controlled copy, and make sure managers know when a change triggers an update.
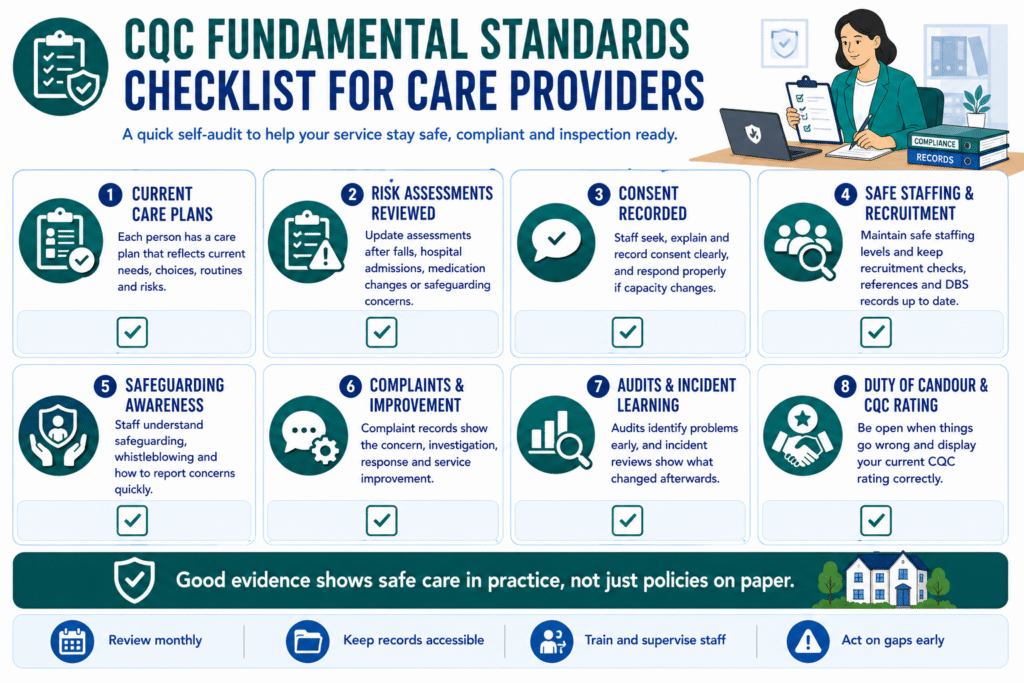
CQC Statement of Purpose Pre-Submission Checklist
Before you send your Statement of Purpose to CQC, check that it gives a clear and accurate picture of your care service.
Use this checklist:
- Our legal business name, address, phone number and email address are correct.
- Our legal status matches our registration application and company records.
- We have listed the correct regulated activities.
- We clearly explain who we support, including age groups and care needs.
- We have stated where we provide or manage care.
- Our service area is specific and realistic.
- Our aims and objectives explain how we will deliver safe, effective, caring, responsive and well-led care.
- We only describe services that our staffing, training, policies and systems can safely support.
- Our registered manager details are accurate and match other CQC paperwork.
- Our Statement of Purpose matches our website, service-user guide, business plan and care policies.
- We have checked spelling, names, addresses and regulated activity wording.
- A manager, director or compliance lead has reviewed the final version.
- We have a process for reviewing the document when the service changes.
A strong Statement of Purpose should give CQC confidence that you understand your service boundaries and can deliver the care you describe. It should also help your care team make safer decisions about referrals, assessments, staffing and support planning.
Final Thoughts: Make Your Statement of Purpose Work for Your Care Business
A strong CQC Statement of Purpose does more than support your registration. It gives your care business a clear foundation.
It tells CQC what you provide, who you support, where you operate, and how your service is managed. It also helps your staff understand the limits of the service, supports safer referrals and keeps your public information consistent.
Keep it factual. Keep it specific. Keep it realistic.
Do not use it to promise every type of care. Use it to describe the service you can deliver safely, confidently and consistently.
If your Statement of Purpose matches your staffing, training, policies, care plans and day-to-day practice, it becomes a useful governance document rather than another piece of registration paperwork.
Need help preparing your CQC Statement of Purpose, registration documents, policies or compliance evidence? Care Sync Experts can support you through the process.
FAQ
What are the 34 CQC quality statements?
The 34 CQC quality statements describe what good care should look like across the five key questions: safe, effective, caring, responsive and well-led. They replaced the older CQC Key Lines of Enquiry (KLOEs) and help CQC assess how providers plan, deliver, monitor and improve care.
For care providers, the important point is not to memorise all 34 statements. You should make sure your policies, staffing, care planning, safeguarding, governance and quality checks show how your service delivers safe, person-centred care in practice.
What are the 5 key lines of CQC?
CQC no longer uses Key Lines of Enquiry, often called KLOEs, as its main assessment framework. It replaced them with quality statements.
However, CQC still uses five core questions to assess care services:
– Is the service safe?
– Is it effective?
– Is it caring?
– Is it responsive to people’s needs?
– Is it well-led?
Providers should use these five questions when checking whether their Statement of Purpose, policies and day-to-day service delivery all work together.
What are the fundamental standards of CQC?
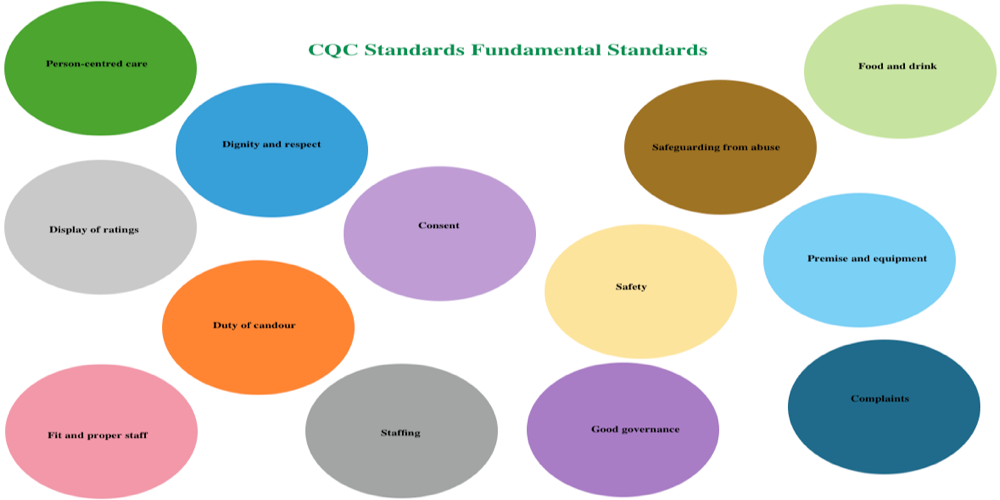
The CQC fundamental standards are the minimum standards below which care must never fall. They cover areas such as person-centred care, dignity and respect, consent, safety, safeguarding, staffing, complaints, good governance and duty of candour.
A CQC Statement of Purpose does not need to repeat every fundamental standard. However, it should describe a service model that supports them. For example, if you say your service provides person-centred care, your assessments, care plans, staff training and review process should show how you deliver that promise.
What are the 6 Cs in care?
The 6 Cs are a care-values framework: care, compassion, competence, communication, courage and commitment. They are not a separate set of CQC regulations, but they remain useful principles for care providers.
You can reflect the 6 Cs in your Statement of Purpose by explaining how you recruit suitable staff, support training and supervision, involve people in care planning, communicate with families and professionals, and respond when care needs change.