The care certificate is a set of 16 standards that define the knowledge, skills, and behaviours every new health and social care worker must demonstrate to deliver safe, compassionate, and person-centred care.
Employers use it as part of induction for roles such as caregivers, support workers, and healthcare assistants. The Care Certificate standards (updated in 2025) ensure you understand essential areas like safeguarding, communication, and duty of care within real care settings.
Key Takeaways
- The care certificate includes 16 Care Certificate standards that every new care worker must complete.
- You can start training through a care certificate online course, but your employer must assess you in the workplace.
- The certificate prepares you for real roles in health and social care, including domiciliary care and care homes.
- It covers key topics like safeguarding, communication, and the duty of care meaning in everyday practice.
- Most employers expect you to complete it during your induction, especially if you are new to social care.
- The certificate does not expire, but you must keep your knowledge updated as standards advance.
What Is the Care Certificate? (For New Caregivers)
If you’re starting a role in care, the care certificate gives you the foundation you need to work safely and confidently from day one.
In simple terms, the care certificate teaches you how to care for people properly. It focuses on real situations you will face every day, supporting vulnerable adults, communicating clearly, protecting people from harm, and delivering respectful, person-centred care.
What is health and social care?
Health and social care covers services that support people’s physical health, mental wellbeing, and daily living needs. This includes:
- Care homes
- Domiciliary (home) care
- Hospitals and community services
What is social care?
Social care focuses on helping people live independently and maintain their quality of life. You may support:
- Older adults
- People with disabilities
- Individuals with mental health needs
As a caregiver, you play a direct role in improving someone’s daily life, not just their health, but their dignity, comfort, and independence.
Why the care certificate matters to you
The care certificate is not just theory. It prepares you for the real responsibilities of care work.
When you complete it, you will:
- Understand your role and responsibilities clearly
- Communicate effectively with service users and colleagues
- Apply safe practices in real care situations
- Deliver care that respects each person’s needs and preferences
Most importantly, it helps you build confidence. You don’t just learn what to do, you learn how to do it properly in real life.
Where it fits in your career
The care certificate is your starting point in health and social care. Many caregivers complete it before moving on to qualifications like NVQ Level 3 Health and Social Care, which develop your skills further and open up career progression opportunities.
If you’re new to the sector, this certificate is your first step into a structured, professional care career.
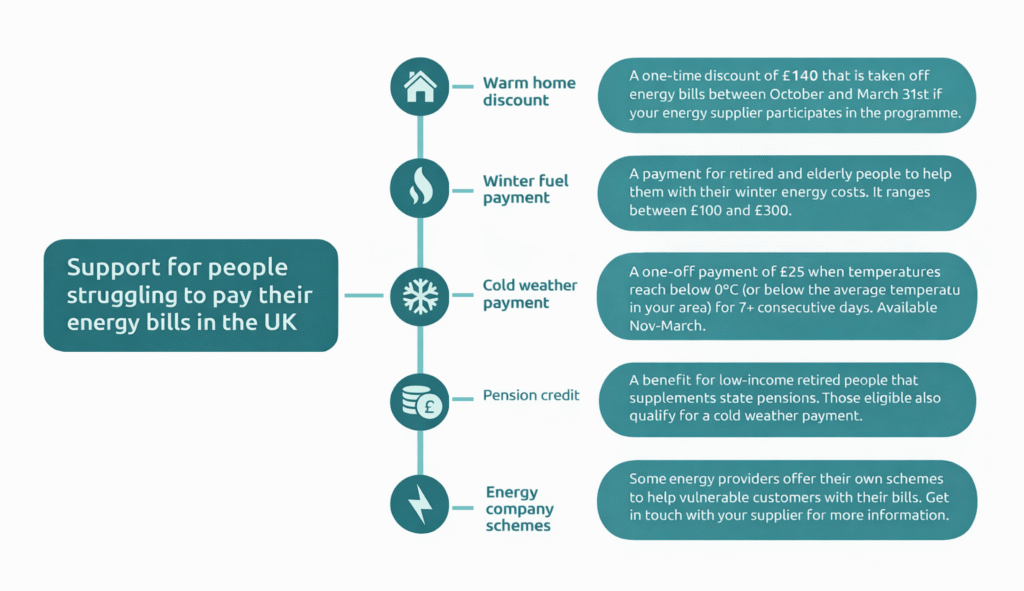
RELATED: What are Cold Weather Payments? Eligibility & How to Claim (2026)
What Are the 16 Care Certificate Standards? (2026 Update)
The Care Certificate standards define what you must know and do to work safely in health and social care. As of 2025, there are 16 standards, including a new addition covering learning disability and autism.
You must complete all 16 standards before your employer signs off your care certificate.
The 16 Care Certificate Standards (Overview)
The standards cover the core areas of health and social care standards:
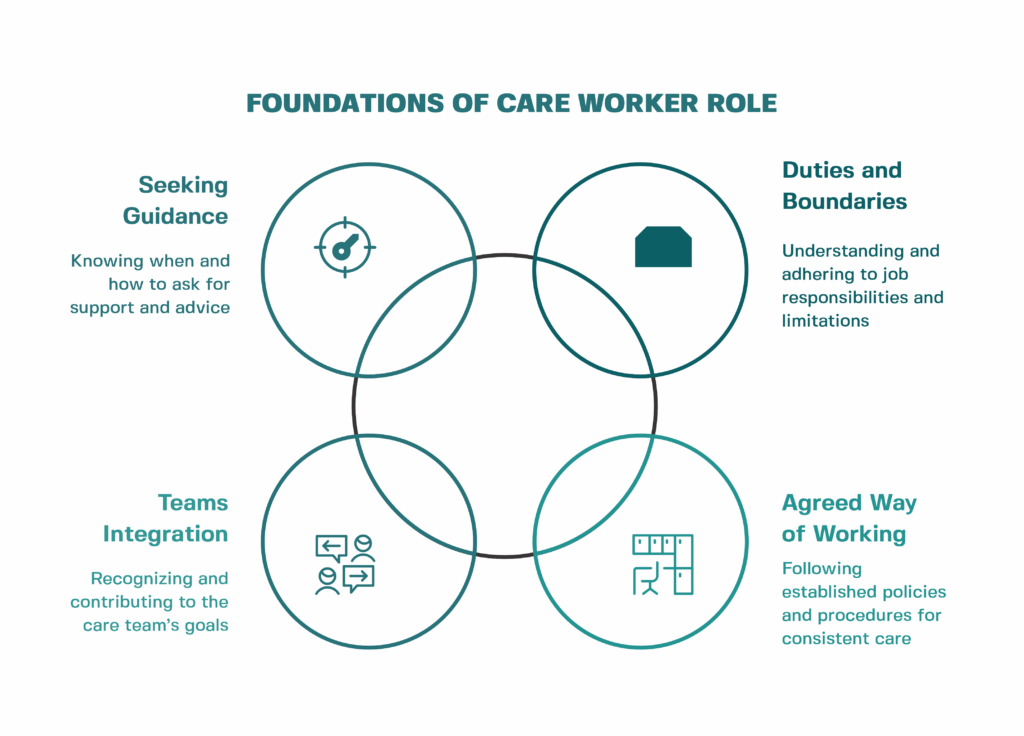
- Understand your role
- Personal development
- Duty of care
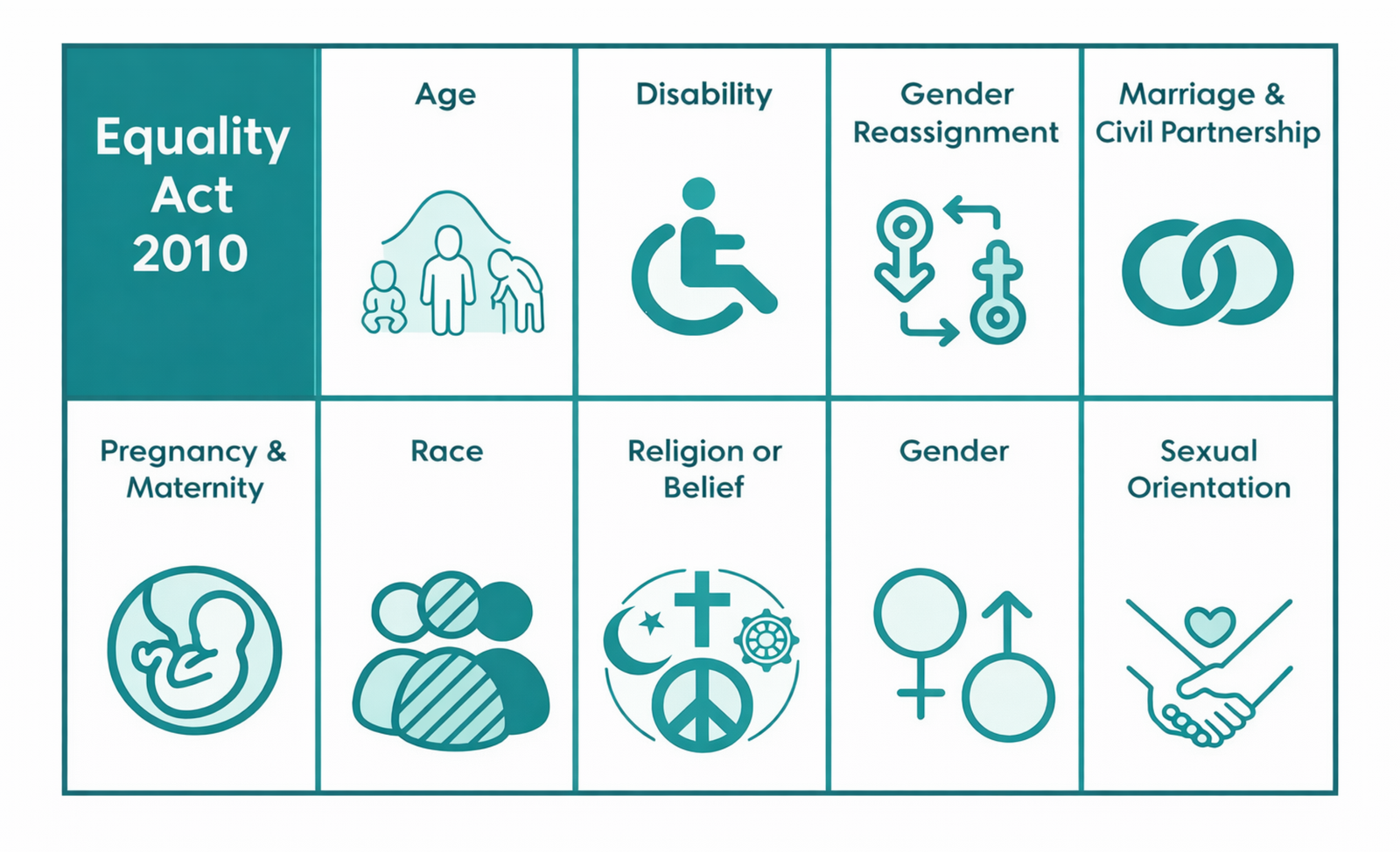
- Equality and diversity
- Work in a person-centred way
- Communication
- Privacy and dignity
- Fluids and nutrition
- Awareness of mental health, dementia, and learning disability
- Safeguarding adults
- Safeguarding children
- Basic life support
- Health and safety
- Handling information
- Infection prevention and control
- Learning disability and autism (new 2025 update)
What these standards mean in real life
Each standard connects directly to what you do every day as a caregiver.
For example:
- Communication helps you build trust with service users
- Safeguarding teaches you how to recognise and report abuse
- Infection control protects both you and the people you care for
You don’t just learn theory, you apply these standards in real care situations
The care certificate ensures that every new worker meets the same baseline across the UK. Employers, regulators, and organisations like the NHS rely on these standards to maintain safe, consistent, and high-quality care.
If you want to work in health and social care, these standards form the foundation of everything you will do moving forward.
Duty of Care Explained (What It Means in Practice)
Understanding duty of care is one of the most important parts of the care certificate. You will use it every day in your role.
What is duty of care?
Duty of care means you must always act in the best interest of the person you support and take reasonable steps to keep them safe from harm.
Duty of care meaning (simple explanation)
The duty of care meaning is straightforward: You have a responsibility to protect people from harm while supporting their rights, dignity, and independence.
Duty of care definition
A clear duty of care definition is: A legal and professional obligation to provide safe, effective, and compassionate care while avoiding actions that could cause harm.
What are the duty of care responsibilities?
As a caregiver, your duty of care includes:
- Keeping service users safe from harm or abuse
- Following care plans and agreed procedures
- Reporting concerns immediately (e.g. safeguarding issues)
- Using equipment safely
- Respecting privacy and dignity
- Acting within your level of training
Real-life example (caregiver perspective)
Imagine you support a service user who refuses medication.
You must:
- Respect their choice
- Explain the risks clearly
- Report the situation to your supervisor
You cannot force them, but you must not ignore the risk either.
This balance between safety and choice sits at the heart of duty of care.
Why duty of care matters in health and social care
In health and social care, your actions directly affect someone’s wellbeing. If you ignore your duty of care, you risk:
- Harm to the service user
- Legal consequences
- Loss of trust from families and employers
The care certificate ensures you fully understand this responsibility before working independently.
Key takeaway
If you remember one thing: Duty of care means doing the right thing, at the right time, to keep people safe while respecting their choices.
This principle guides everything you do as a caregiver.
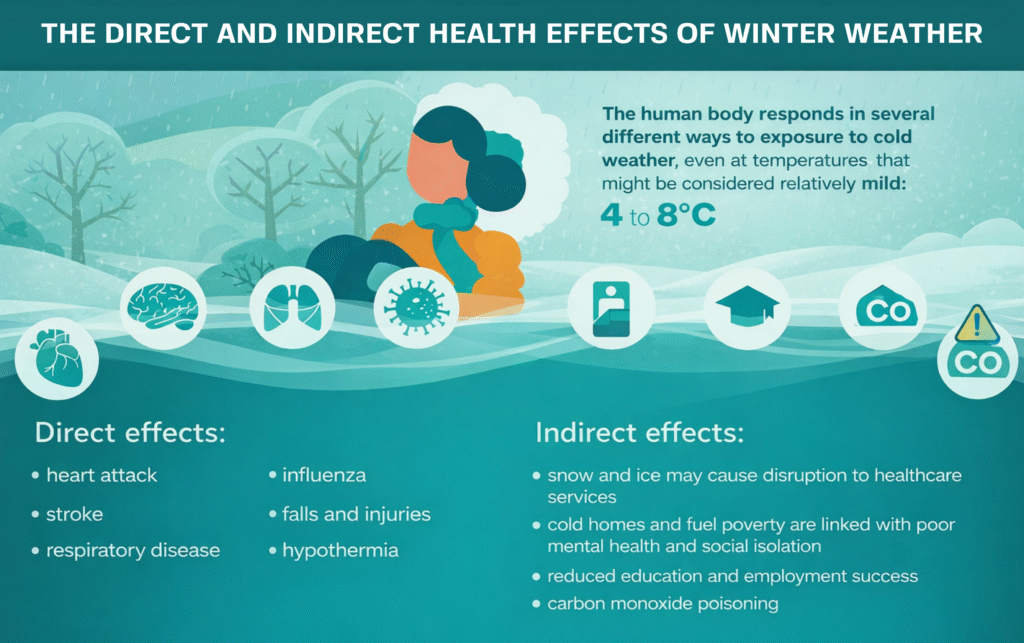
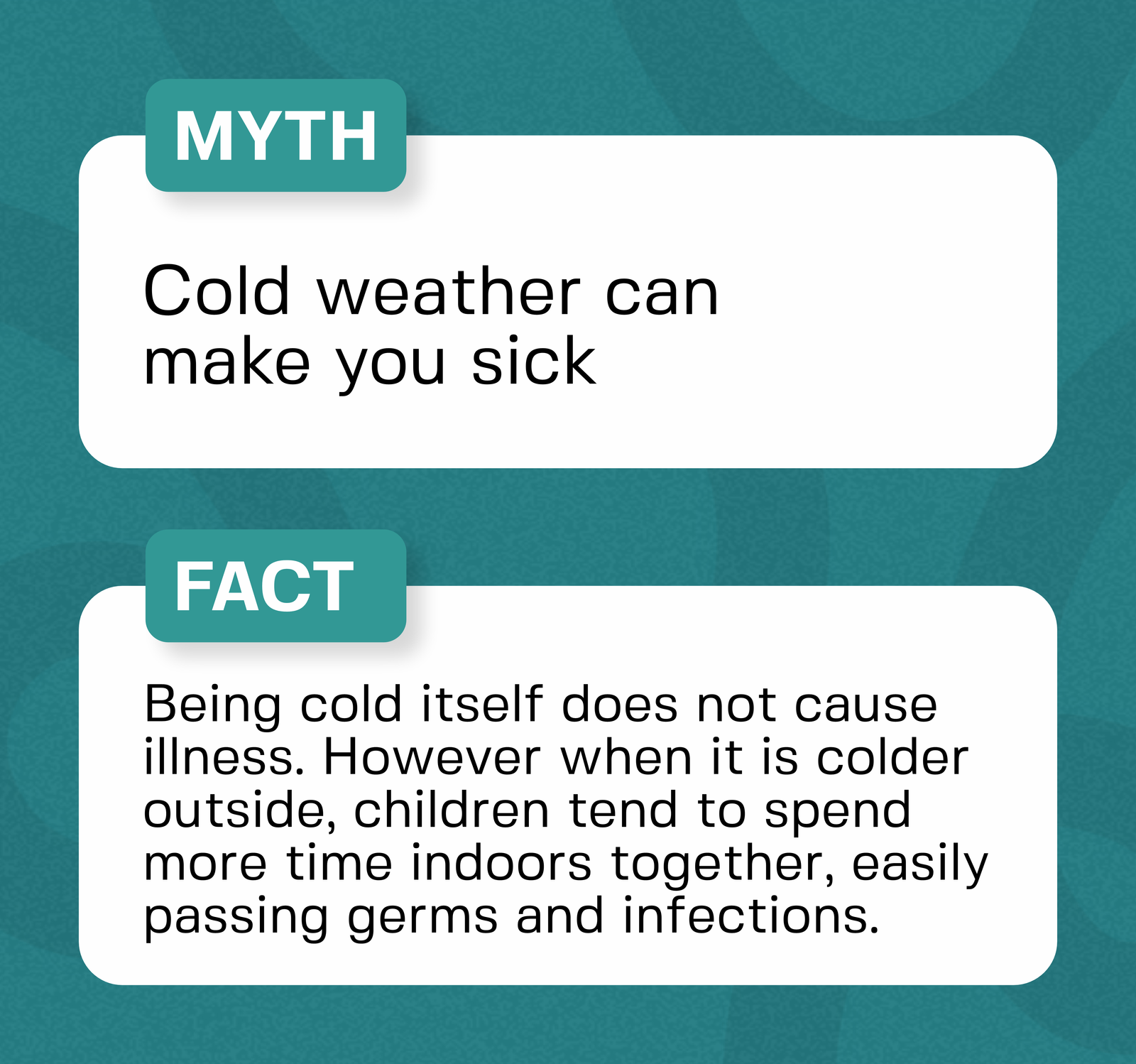
READ MORE: Does Cold Weather Make You Sick? The Complete 2026 Guide
Who Needs the Care Certificate?
If you’re starting a role in care, you will almost always need the care certificate. Employers use it to make sure every new worker meets the same health and social care standards before working independently.
You need the care certificate if you are:
- A caregiver in a care home or domiciliary (home care) setting
- A healthcare assistant in a hospital or community service
- A support worker helping people with disabilities or mental health needs
- New to health and social care with little or no prior experience
Most employers include the care certificate as part of your induction training.
Why employers expect it
Care providers must show regulators (like the CQC) that their staff are trained and competent. The care certificate helps them prove that.
When you complete it, you show that you can:
- Deliver safe care
- Follow procedures correctly
- Understand your responsibilities
This makes you more employable and trusted in your role.
If you’re applying from overseas
If you plan to work in the UK under a health and care worker visa, employers will often expect you to complete the care certificate shortly after you start work.
While the certificate is not a visa requirement, it:
- Helps you adapt to UK care standards
- Shows you understand local expectations
- Improves your chances of long-term employment
Do experienced workers need it?
If you already work in care and hold qualifications like NVQ Level 3 Health and Social Care, your employer may not require you to complete the full care certificate again.
However, some organisations still use it to:
- Standardise training
- Refresh knowledge
- Ensure compliance with updated standard
How to Get a Care Certificate (NHS & Online)
You don’t apply for the care certificate like a normal course. You earn it while working in a real care role.
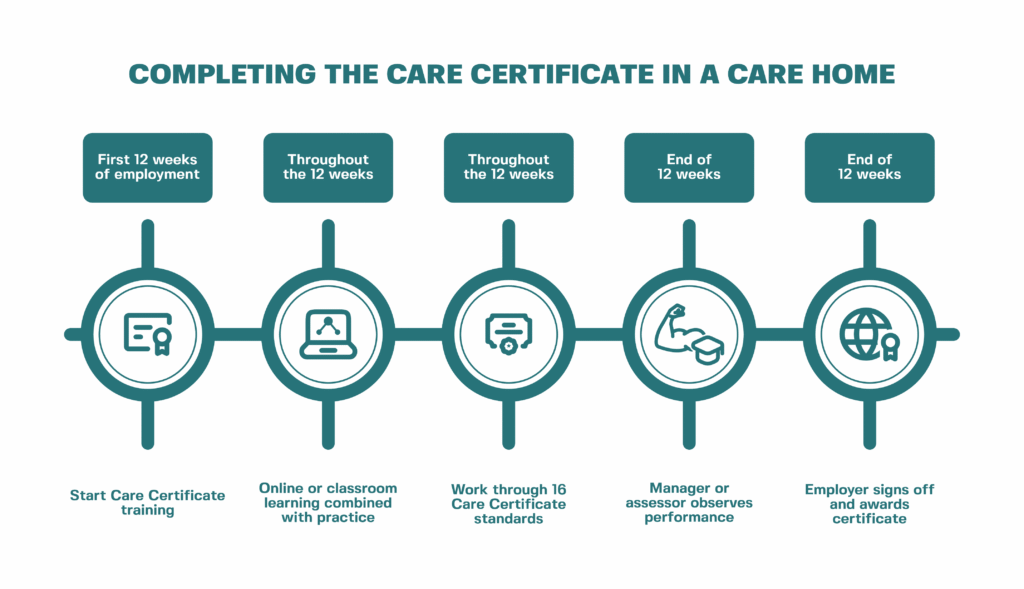
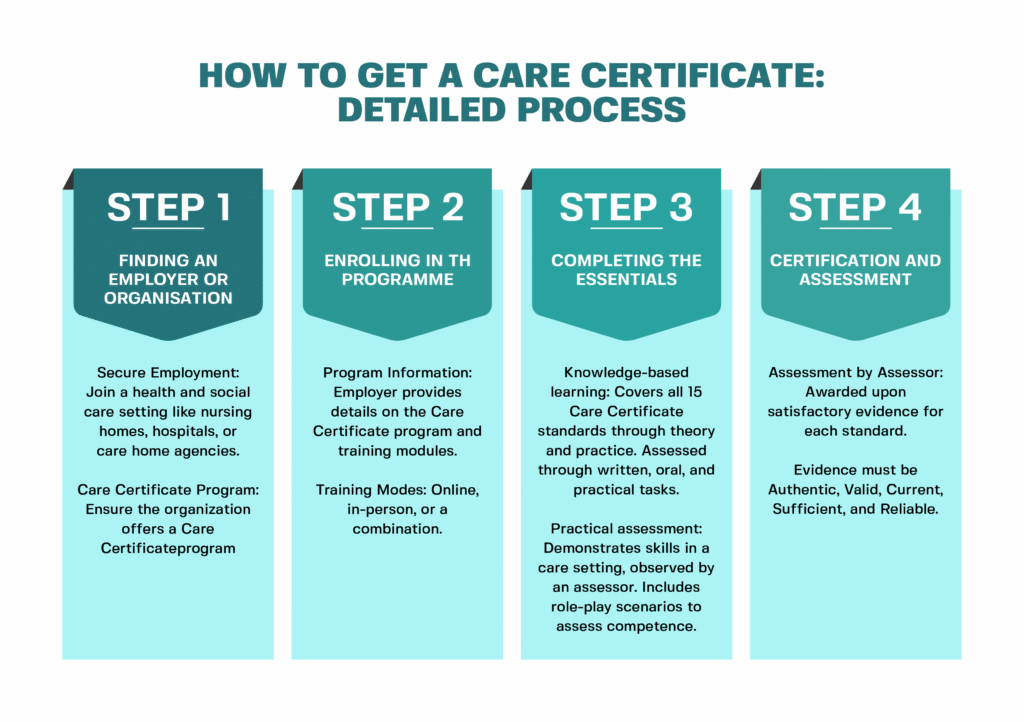
Step-by-step: How to get a Care Certificate NHS online
- Start a care job
Join a role such as a caregiver, support worker, or healthcare assistant.
- Begin a Care Certificate course
Your employer will enrol you in training. This may include an Elfh Care Certificate programme or another care certificate online provider.
- Complete the training workbook
You will study topics based on the Care Certificate standards, including safeguarding, communication, and duty of care.
- Apply your learning in the workplace
You must demonstrate what you’ve learned while working with service users.
- Get assessed by your employer
A supervisor or assessor will observe your work and confirm your competence.
- Receive your certificate
Once you complete all 16 standards and pass assessment, your employer signs off your care certificate.
Important: Online training alone is not enough
You can take a care certificate online course, but this only covers the theory.
To fully achieve the certificate:
- You must work in a real care setting
- An assessor must sign off your practical skills
This is why many people search for Care Certificate answers, but in reality, you must demonstrate understanding, not just complete quizzes.
Where NHS training fits in
Many organisations use NHS-supported platforms like the Elfh Care Certificate (e-Learning for Healthcare).
This training:
- Covers the theoretical part of all standards
- Aligns with NHS and Skills for Care guidance
- Supports your induction
However, your employer still completes the final assessment in the workplace.
Key takeaway
You get the care certificate by combining training with real work experience, not by completing an online course alone.
This approach ensures you can actually deliver safe, effective care in real-life situations.
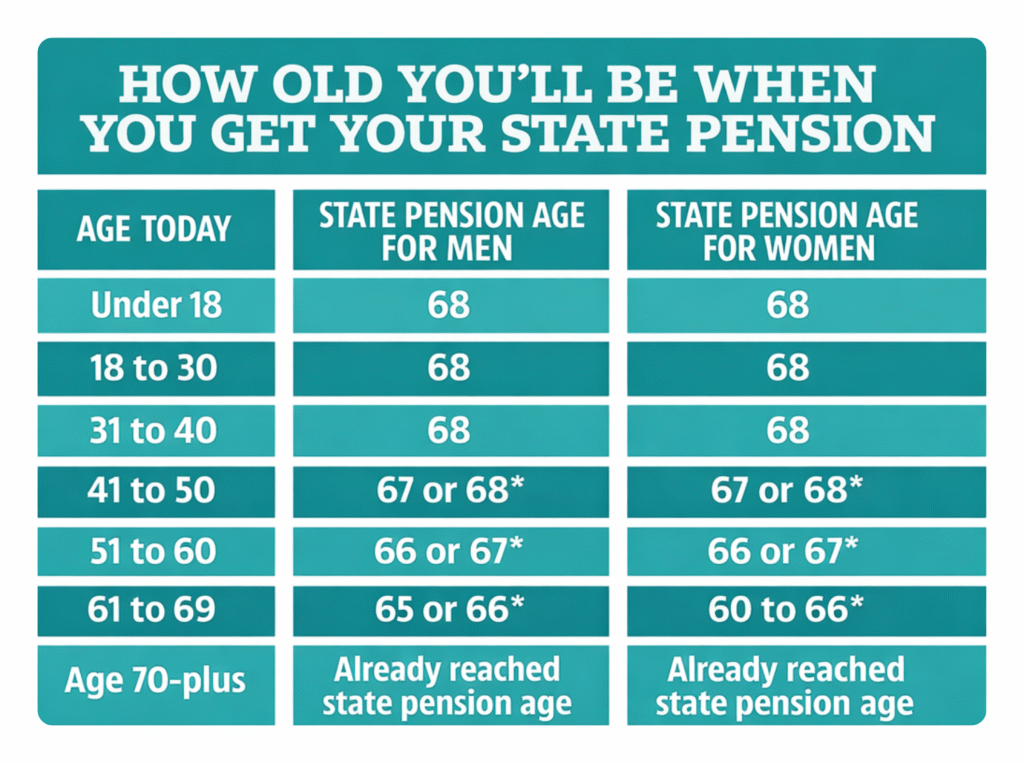
SEE ALSO: What Is the Retirement Age in the UK? (2026 Guide for Care Workers & Providers)
Care Certificate Online vs Workplace Assessment
Many new caregivers assume they can complete the care certificate online and receive the certificate immediately. In reality, it doesn’t work that way.
What a care certificate online course actually does
A care certificate online course helps you learn the theory behind the Care Certificate standards. It usually includes:
- Videos and reading materials
- Quizzes or workbook-style questions
- Guidance on topics like safeguarding and duty of care
This training builds your knowledge, but it does not mean you have completed the full care certificate.
Why workplace assessment is required
To achieve the care certificate, you must prove that you can apply your knowledge in real situations.
An assessor (usually your manager or supervisor) will:
- Observe how you support service users
- Check how you communicate and follow care plans
- Confirm you meet each of the 16 standards in practice
This step is mandatory. No provider can issue a valid certificate without it.
The truth about “Care Certificate answers”
Many people search for Care Certificate answers online. However:
- There are no official answers you can copy
- Each employer expects you to demonstrate real understanding
- Assessors focus on how you apply knowledge, not just what you write
If you rely only on answers, you won’t pass the practical assessment.
Simple breakdown
| Training Type | What You Get |
| Care certificate online | Knowledge and theory |
| Workplace assessment | Practical competence |
| Both combined | Full care certificate |
Key takeaway
You can learn the care certificate online, but you must prove your skills in the workplace to achieve it.
This ensures every caregiver can deliver safe, consistent, and high-quality care in real-life settings.
How Long Does It Take and How Much Does It Cost?
Before you start, you’ll want to know how long the care certificate takes and whether you need to pay for it.
How long does the care certificate take?
Most caregivers complete the care certificate within 6 to 12 weeks during their induction.
However, the timeline depends on:
- Your employer’s training schedule
- Your working hours
- How quickly you complete each standard
If you study through a care certificate online course, you can complete the theory in a few hours or days.
But the full certificate takes longer because you must complete workplace assessments.
How much does the care certificate cost?
In most cases, you don’t pay for the care certificate.
Employers usually cover:
- Training
- Assessment
- Certification
If you choose a private Care Certificate course, prices typically range from £15 to £50 depending on the provider.
Free vs paid training
- Free options:
NHS-aligned platforms like the Elfh Care Certificate offer free training modules.
- Paid options:
Platforms like Caredemy or CPD Online College provide structured courses and certificates of completion.
Remember: paying for a course does not replace workplace assessment.
What affects the total cost?
Even if the course is free, your employer invests in:
- Staff time for supervision
- Assessment and sign-off
- Ongoing training
That’s why most employers include the care certificate as part of your job training.
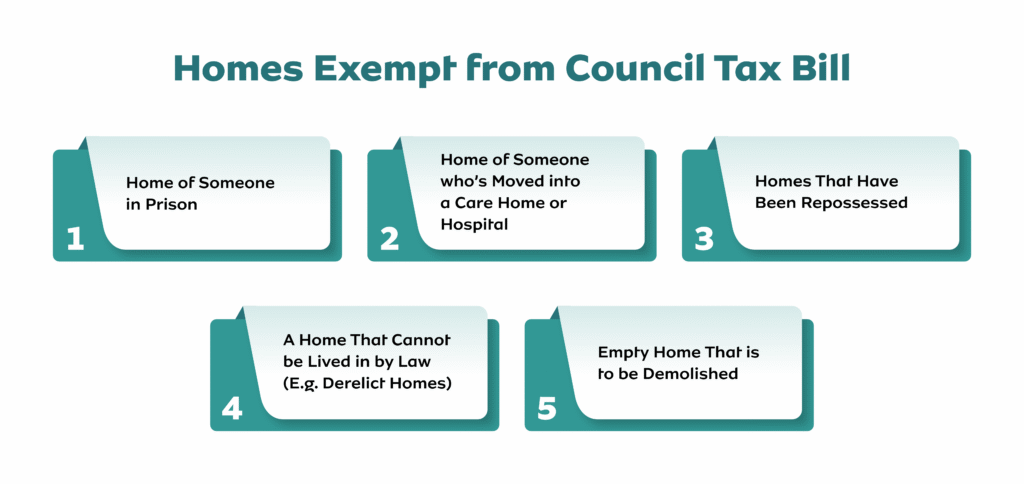
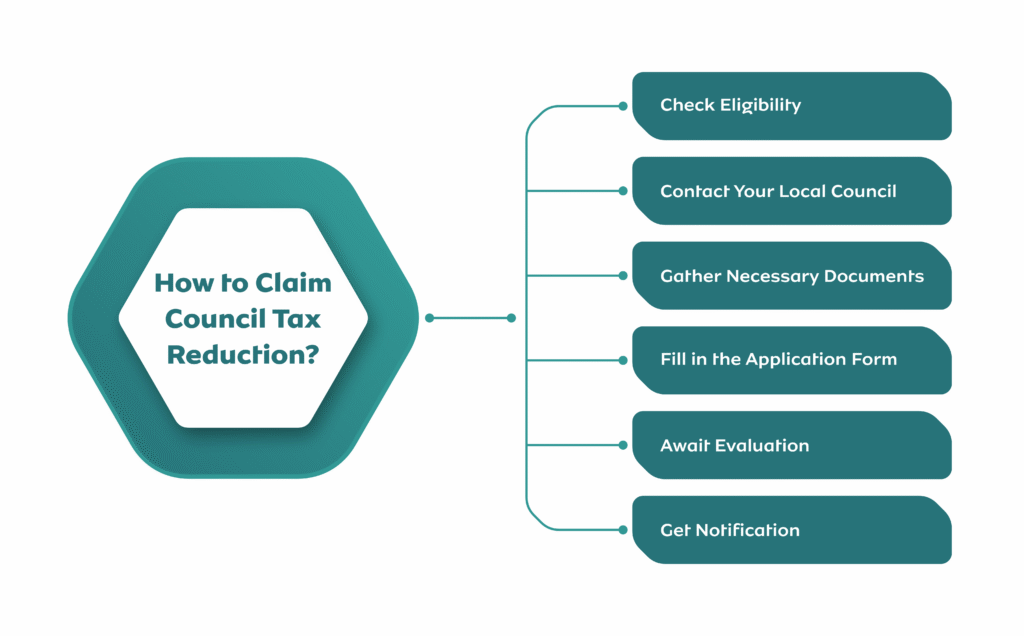
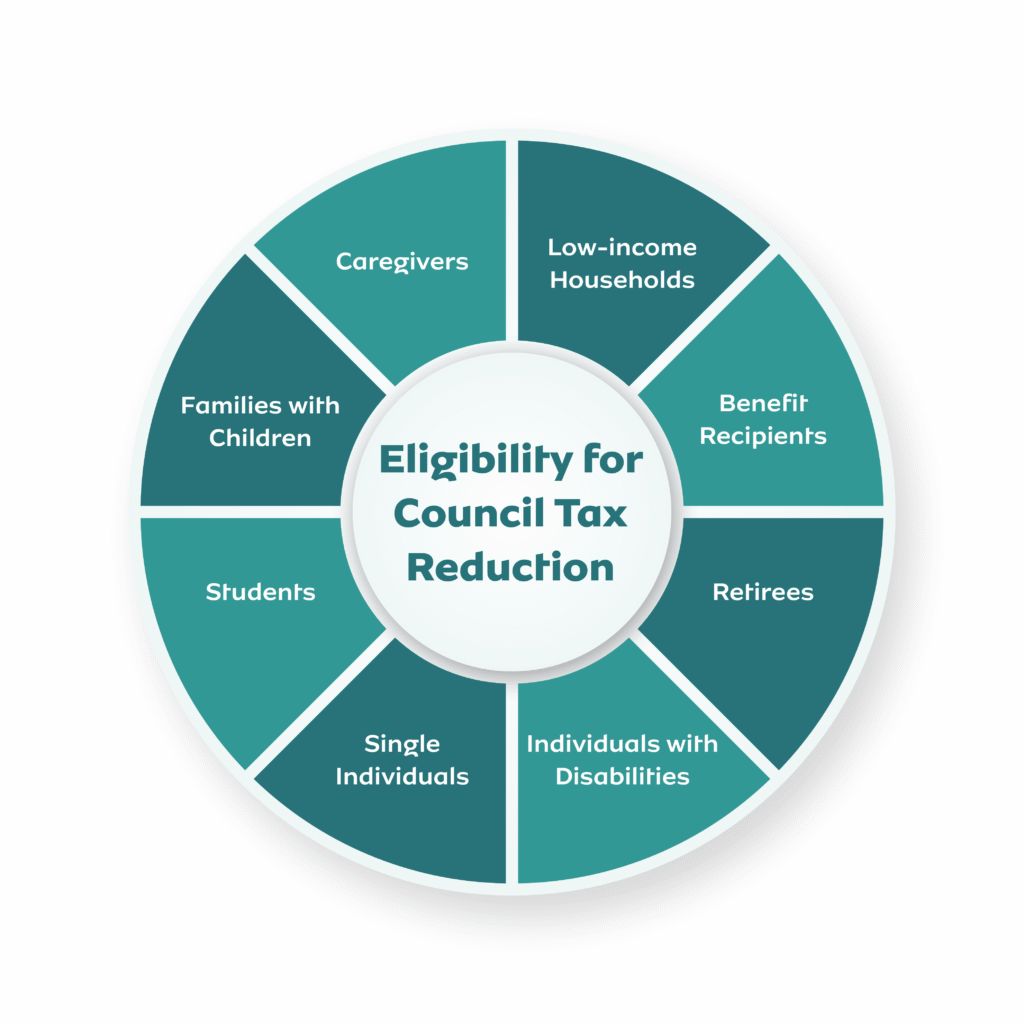
MORE: What Disabilities Qualify for Council Tax Reduction? 2026
Where to Find Care Certificate Training
You can start learning the care certificate through several trusted providers. Most employers will guide you, but it helps to know your options
1. NHS e-Learning (Elfh Care Certificate)
The Elfh Care Certificate (e-Learning for Healthcare) is one of the most widely used platforms in the UK.
It:
- Covers all Care Certificate standards
- Aligns with NHS and Skills for Care guidance
- Offers free, structured online modules
Many care providers use this as part of staff induction.
2. Skills for Care (Official Resources)
Skills for Care provides the official framework, guidance, and materials.
You can access:
- Workbooks and guides (care certificate download)
- Assessment templates
- Employer resources
These materials support both learners and assessors.
3. Online Training Providers
Several platforms offer paid care certificate online courses:
- Caredemy
- CPD Online College
These providers:
- Deliver structured lessons
- Provide certificates of completion
- Help you prepare for workplace assessment
Useful if you want to learn before starting a job.
Important: Choose the right path
Before enrolling, remember:
- Online courses only cover theory
- You still need employer assessment to complete the care certificate
- Employers may prefer specific training providers
Care Certificate Answers (What You Should Know)
Many new caregivers search for Care Certificate answers online, especially when completing workbooks or quizzes. It’s important to understand how this actually works.
Are there official Care Certificate answers?
No, there are no official Care Certificate answers you can copy and submit.
The care certificate focuses on:
- Your understanding
- Your ability to apply knowledge
- Your performance in real care situations
This means assessors look beyond written responses.
Why copying answers won’t help
Even if you find care certificate answers online:
- Your employer will assess you in real situations
- You must explain your decisions and actions
- You need to show safe and correct practice
If you don’t understand the content, you won’t pass the assessment.
What assessors actually expect
Your assessor wants to see that you can:
- Explain your actions clearly
- Follow care procedures correctly
- Apply the duty of care in real situations
- Communicate effectively with service users
They may:
- Observe you during care tasks
- Ask questions about your decisions
- Review your workbook responses
The best way to complete your workbook
Instead of searching for answers, focus on:
- Understanding each standard
- Using real examples from your work
- Writing in your own words
- Asking your supervisor when unsure
This approach helps you pass both the written and practical parts.
READ: Bereavement Support Payment (BSP) in the UK: Who Qualifies, How Much You Get, and How to Apply
Is the Care Certificate Mandatory?
The care certificate is not a legal requirement, but most employers expect you to complete it if you are new to health and social care.
Is it required by law?
No, the care certificate is not required by law.
However:
- The Care Quality Commission (CQC) expects providers to train staff properly
- Employers must show that workers are competent and safe
The care certificate helps them meet these expectations.
Why employers require it
Most care providers include the care certificate as part of your induction because it:
- Sets a consistent standard across the workforce
- Ensures you understand the Care Certificate standards
- Reduces risk to service users
- Supports compliance with health and social care standards
In practice, it becomes mandatory within the organisation, even if not required by law.
What happens if you don’t complete it?
If you refuse or fail to complete the care certificate:
- Your employer may not allow you to work independently
- You may struggle to pass probation
- It could affect your job security
Employers rely on it to confirm your competence.
Is it required for a health and care worker visa?
The care certificate is not a direct requirement for a health and care worker visa, but:
- Employers often expect you to complete it after hiring
- It helps you meet UK care standards
- It improves your long-term employability
Does the Care Certificate Expire?
The care certificate does not expire once you complete it. You keep it as a permanent record of your training and competence.
Do you need to renew it?
No, you do not need to renew the care certificate.
However, you must:
- Keep your knowledge up to date
- Follow current health and social care standards
- Complete additional training when required
Care practice evolves, so your skills must stay current.
Even though the certificate stays valid, employers expect you to continue learning.
You may need to refresh:
- Safeguarding procedures
- Infection control practices
- Updates to the Care Certificate standards
This ensures you continue to provide safe and effective care.
What happens if you change jobs?
When you move to a new employer:
- Your care certificate still counts
- You may need to complete a refresher or workplace assessment
- Employers may check your previous training records
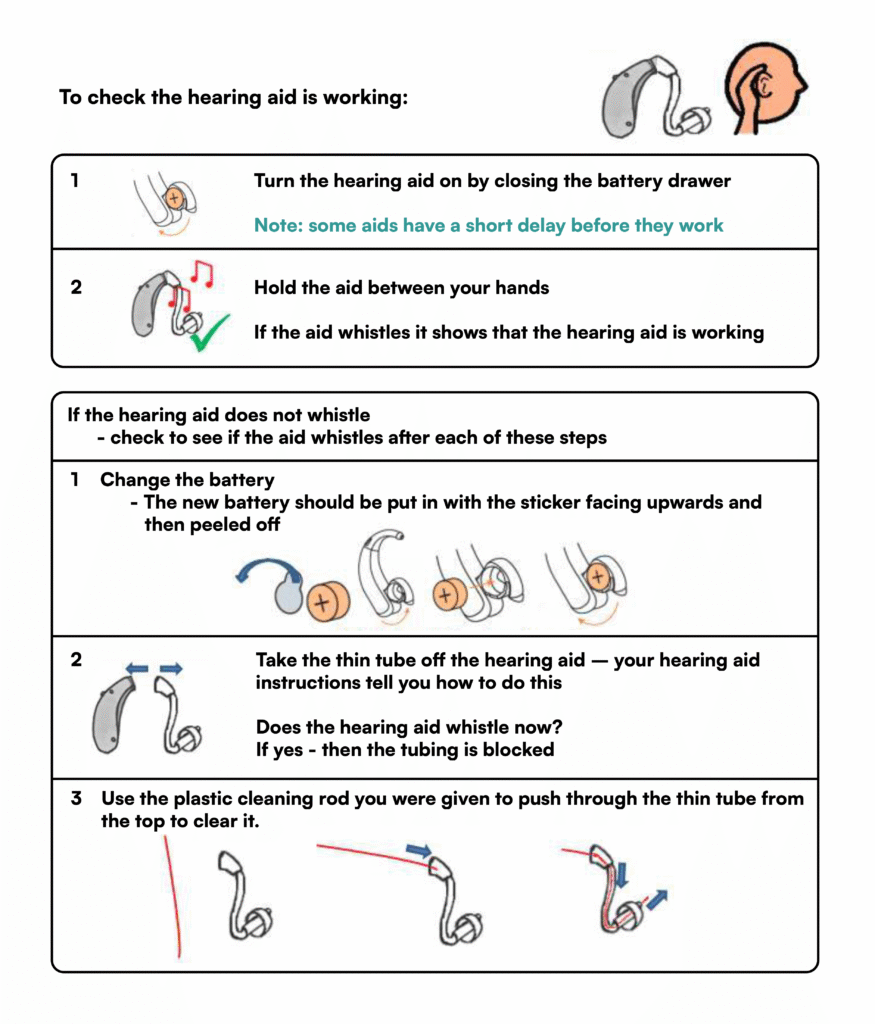
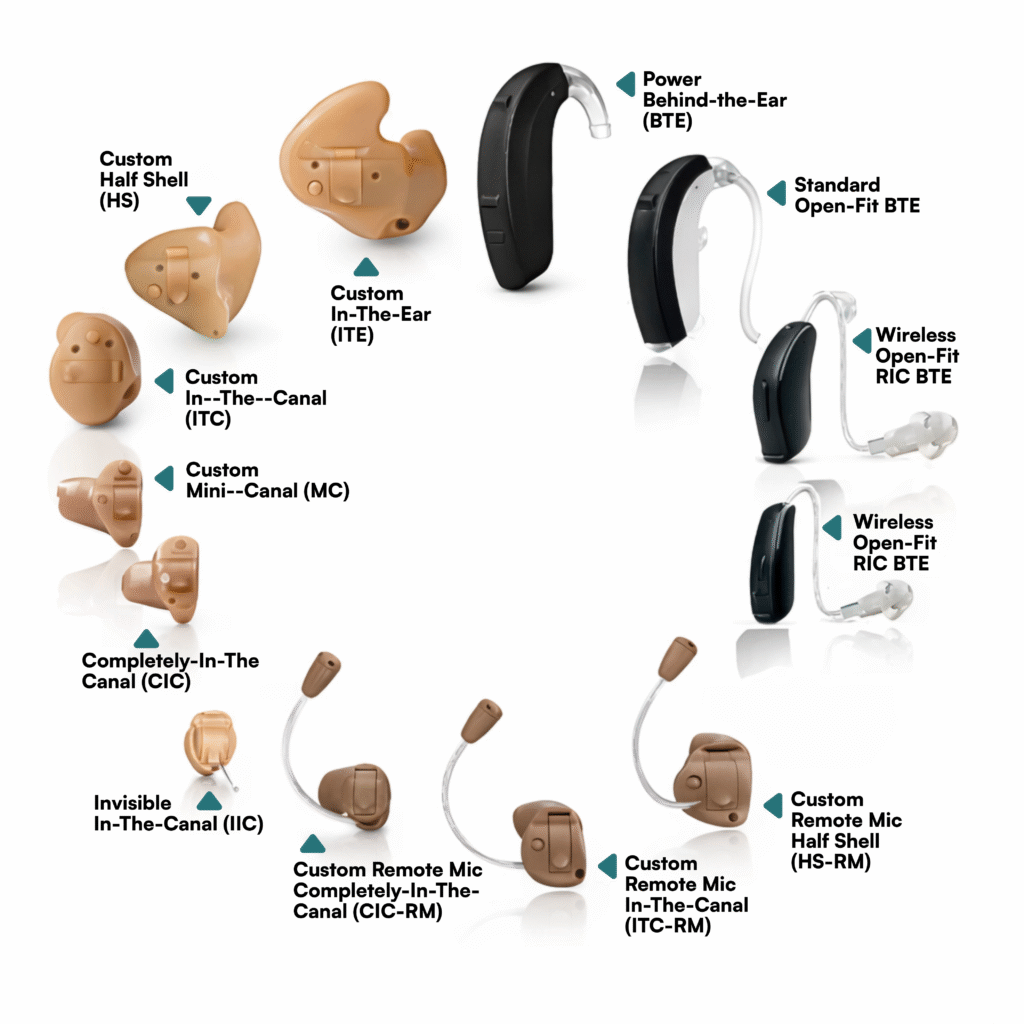
ALSO: NHS Hearing Aids UK: Cost, Types, Waiting Times, and How to Get One in 2026
Care Certificate vs NVQ Level 3 Health and Social Care
Many caregivers ask whether the care certificate is the same as NVQ Level 3 Health and Social Care. They are not the same, they serve different purposes.
What is the difference?
| Care Certificate | NVQ Level 3 Health and Social Care |
| Entry-level training | Advanced qualification |
| Completed during induction | Completed after gaining experience |
| Focuses on basic skills and safety | Focuses on deeper knowledge and responsibility |
| Mandatory (in practice) for new staff | Optional but recommended for career growth |
What the care certificate does
The care certificate helps you:
- Understand the Care Certificate standards
- Learn the basics of health and social care
- Work safely under supervision
It prepares you to start your role.
What NVQ Level 3 does
NVQ Level 3 Health and Social Care helps you:
- Take on more responsibility
- Develop advanced care skills
- Progress into senior roles
It builds on what you learned during the care certificate.
Which one should you choose?
If you are new to care:
- Start with the care certificate
If you already have experience:
- Progress to NVQ Level 3 Health and Social Care
How they work together
Think of it like this:
The care certificate gets you started.
NVQ Level 3 helps you grow your career.
Many employers expect you to complete both over time.
Should You Take the Care Certificate?
If you are new to health and social care, you should complete the care certificate as soon as you start working.
You should take it if:
- You are starting your first care role
- You want to understand UK care standards
- You plan to build a long-term career in care
You may not need it if:
- You already hold qualifications like NVQ Level 3 Health and Social Care
- You have proven experience and employer sign-off
Most employers will still expect you to complete it.
Conclusion
Starting a career in care can feel overwhelming, especially when you’re expected to understand regulations, responsibilities, and real-life care situations from day one. The care certificate simplifies that journey. It gives you a clear foundation, builds your confidence, and prepares you to deliver safe, compassionate, and person-centred care in real environments.
Whether you’re supporting someone in their home, working in a care facility, or beginning your journey in health and social care, the care certificate helps you do your job properly, not just follow instructions, but truly understand the impact of your actions.
As the sector continues to evolve, one thing remains constant: well-trained caregivers provide better outcomes, build stronger trust, and create safer care environments. The care certificate is where that standard begins.
Need Expert Support Navigating Care Training, Compliance, and Career Progression?
Care Sync Experts supports caregivers, care providers, and healthcare organisations across the UK with clear, practical guidance on care training, compliance, and professional development in health and social care.
From helping new caregivers understand the care certificate, workplace assessments, and duty of care, to guiding organisations on compliance, training frameworks, and operational best practices, our specialists turn complex requirements into simple, actionable steps.
Whether you need support completing your care certificate, improving staff training, or aligning your organisation with Care Certificate standards and CQC expectations, our team delivers tailored guidance designed for real-world care settings.
Build your confidence, strengthen your care delivery, and stay compliant with evolving UK care standards.
Contact Care Sync Experts today to get expert support on care training, compliance, and building a successful career in health and social care.
FAQ
What jobs can you get with a care certificate in the UK?
With a care certificate, you can apply for entry-level roles in health and social care, including:
– Care assistant (care homes or domiciliary care)
– Support worker (mental health or disability services)
– Healthcare assistant (NHS or private settings)
– Personal care assistant
These roles allow you to gain experience and progress to higher qualifications like NVQ Level 3 Health and Social Care.
What is the care certificate equivalent to in the UK?
The care certificate is not a formal qualification like a diploma or NVQ. Instead, it is an industry-recognised standard for induction training in health and social care.
Think of it as:
– A foundation level requirement for new care workers
– A stepping stone before moving on to qualifications like NVQ Level 2 or Level 3
It proves competence, not academic achievement.
How much is a Care Worker’s salary in the UK?
Care worker salaries in the UK vary depending on experience, location, and employer.
On average:
– Entry-level care workers earn £20,000–£24,000 per year
– Experienced workers can earn £25,000–£30,000+
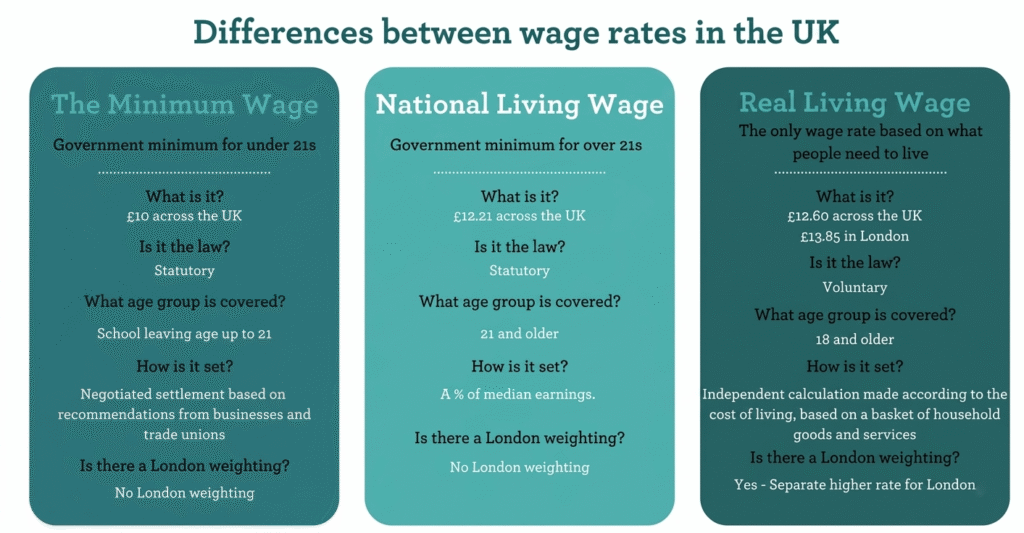
– Hourly rates typically range from £10 to £15 per hour
– Higher pay is possible with experience, specialist roles, or additional qualifications.
What qualifications do I need to be a care worker in the UK?
You do not need formal qualifications to start a care role, but employers expect you to complete the care certificate during your induction.
To progress in your career, you may need:
– NVQ Level 2 or 3 Health and Social Care
– Specialist training (e.g., dementia care, safeguarding)
– Ongoing professional development
The care certificate is your entry point, while further qualifications help you grow into senior roles.