If you need the number for PIP payment enquiries, you can contact the Department for Work and Pensions (DWP) using the official PIP enquiry line below. These numbers help you check an existing claim, report PIP changes, or ask about payments.
PIP Contact Number (Existing Claims and Payments)
- PIP contact number (existing claim): 0800 121 4433
- Textphone / Relay UK: 0800 121 4493
- Opening hours: Monday to Friday, 9am–5pm
Use this pip contact number 0800 if you need to:
- Check the status of your claim
- Ask about PIP payments backdated
- Report PIP changes such as a change of address or health condition
- Ask questions about your award or assessment outcome
Many people search for the number for personal independence payment or the dept work and pensions tel no when they need help with a claim. The number above connects you directly to the PIP enquiry line managed by the Department for Work and Pensions.
PIP Contact Number (New Claims)
To start a new claim, call the DWP contact number below:
- New PIP claims: 0800 917 2222
- Opening hours: Monday to Friday, 8am–5pm
When you call this dept of work and pensions contact no, an advisor will ask for basic information and begin your claim for Personal Independence Payment. After the call, the DWP sends you the form called “How Your Disability Affects You.”
Northern Ireland PIP Contact Numbers
If you live in Northern Ireland, contact the Department for Communities instead of the DWP:
- Existing claims / payments: 0800 587 0932
- New claims: 0800 012 1573
When to Use the PIP Enquiry Line
You should call the pip enquiry line if you need help with:
- Checking PIP payment dates
- Reporting a change of circumstances
- Asking about PIP extensions in the UK
- Updating your personal details
- Understanding a decision letter
- Fixing payment problems
Many caregivers contact the DWP contact number 0800 on behalf of family members who cannot manage their claim alone.
If your question relates to a medical assessment, the DWP may ask you to contact the assessment provider directly (such as Capita, Ingeus, or Maximus).
What Personal Independence Payment (PIP) Is and Who It Helps
Personal Independence Payment (PIP) is a UK government benefit that helps people aged 16 to State Pension age cover the extra costs of living with a long-term health condition or disability. The Department for Work and Pensions (DWP) manages PIP in England and Wales, while different systems apply in Scotland and Northern Ireland.
Unlike many benefits, PIP is not means-tested. Your income, savings, or employment status do not affect whether you can receive it. Many people continue working while receiving PIP because the benefit focuses on how your condition affects your daily life, not how much money you earn.
PIP exists to support people who struggle with everyday tasks or mobility because of a physical, mental, or neurological condition. This can include people living with conditions such as arthritis, multiple sclerosis, anxiety disorders, or ADHD PIP claims, where attention and executive function difficulties affect daily activities.
Caregivers often play a key role in the process. Many families help a relative manage their claim, contact the pip enquiry line, gather medical evidence, and communicate with the Department for Work and Pensions contact number when changes happen. Understanding how PIP works helps caregivers support someone through the application, assessment, and payment process.
PIP contains two main components:
Daily Living Component
This part supports people who need help with everyday activities such as:
- Preparing and eating food
- Washing and bathing
- Dressing and undressing
- Managing medication or treatment
- Communicating with others
- Managing money
Mobility Component
This part helps people who struggle with getting around, including:
- Planning and following a journey
- Leaving the home safely
- Walking or moving around
You may receive one component or both, depending on how your condition affects your independence.
Many families also ask what other benefits can I claim with PIP because receiving PIP can unlock additional financial support, mobility schemes, and caregiver benefits. We will explain those options later in this guide.
Before applying, it is important to understand Personal Independence Payment eligibility, because the DWP bases every decision on how your condition affects daily living and mobility rather than the medical diagnosis itself.
RELATED: What Is the Carers Element Universal Credit? 2026
Personal Independence Payment Eligibility: Who Can Claim PIP?
To qualify for Personal Independence Payment (PIP), you must meet several criteria set by the Department for Work and Pensions (DWP). These rules focus on how your health condition affects your daily life, not simply on the condition itself. Understanding Personal Independence Payment eligibility helps you decide whether it is worth starting a claim.
Age Requirement
You can usually claim PIP if you:
- Are 16 years old or over
- Have not yet reached State Pension age
If you are already receiving PIP when you reach State Pension age, your payments normally continue as long as your circumstances remain the same.
Health Condition or Disability
You must have a long-term physical or mental health condition or disability that affects your ability to carry out everyday activities or move around.
Examples include:
- Mobility impairments
- Chronic illnesses
- Neurological conditions
- Mental health conditions
- ADHD PIP claims, where attention or executive function issues affect daily living
The DWP does not award PIP based on the diagnosis alone. Instead, they assess how the condition affects your independence and daily functioning.
Duration Rule
Your condition must meet the qualifying period rule:
- You must have experienced difficulties for at least 3 months, and
- Those difficulties must be expected to continue for at least 9 more months
This rule ensures PIP supports people with long-term needs rather than short-term illness or injury.
Daily Living or Mobility Difficulties
The DWP evaluates whether you need help with:
Daily living activities such as:
- Preparing food
- Washing or bathing
- Dressing
- Managing medication
- Communicating with others
Mobility activities such as:
- Planning and following journeys
- Physically moving around
During the assessment process, a health professional assigns points for different activities. Your total score determines whether you qualify for the standard or enhanced rate of PIP.
Residency Requirements
You must normally:
- Live in England, Wales, or Northern Ireland
- Have lived in the UK for a certain period before claiming
Rules differ slightly depending on your situation.
For example, people living in Scotland usually apply for Adult Disability Payment instead of PIP, which we will explain later in the guide.
Supporting Evidence Matters
Your claim becomes much stronger if you include supporting evidence, such as:
- Letters from doctors or specialists
- Care plans or treatment records
- Statements from caregivers or family members
- Prescriptions or medical reports
This evidence helps the DWP understand how your condition affects your daily life before they schedule an assessment.
Once you understand Personal Independence Payment eligibility, the next step is learning how to apply for Personal Independence Payment, which we will explain step by step in the next section.
READ MORE: What Is Person Centred Care? 2026 Guide
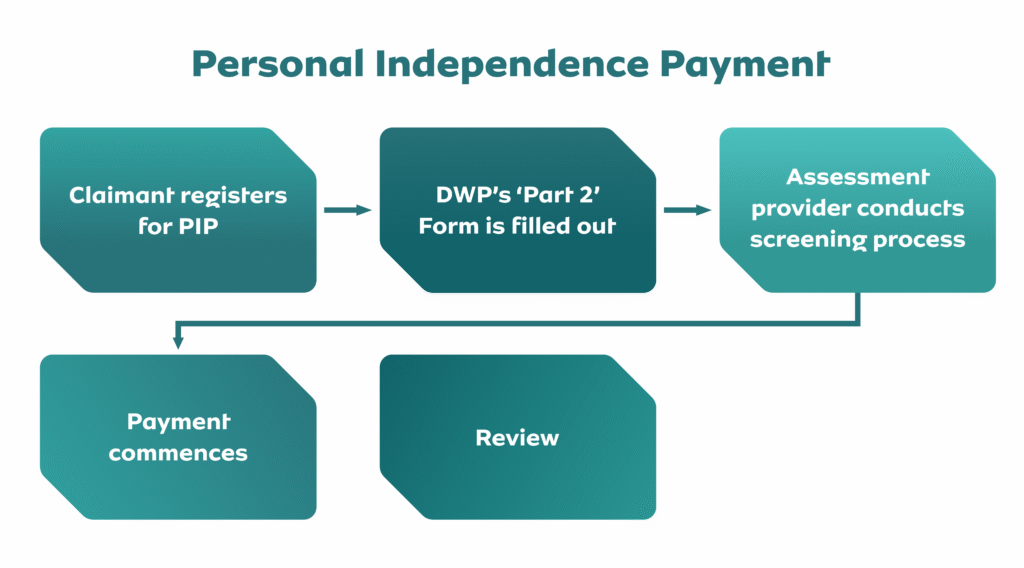
How to Apply for Personal Independence Payment (Step-by-Step)
If you meet Personal Independence Payment eligibility, the next step is to start the claim with the Department for Work and Pensions (DWP). Many caregivers help family members complete this process, especially when the person claiming struggles with paperwork or phone calls.
The process happens in several stages.
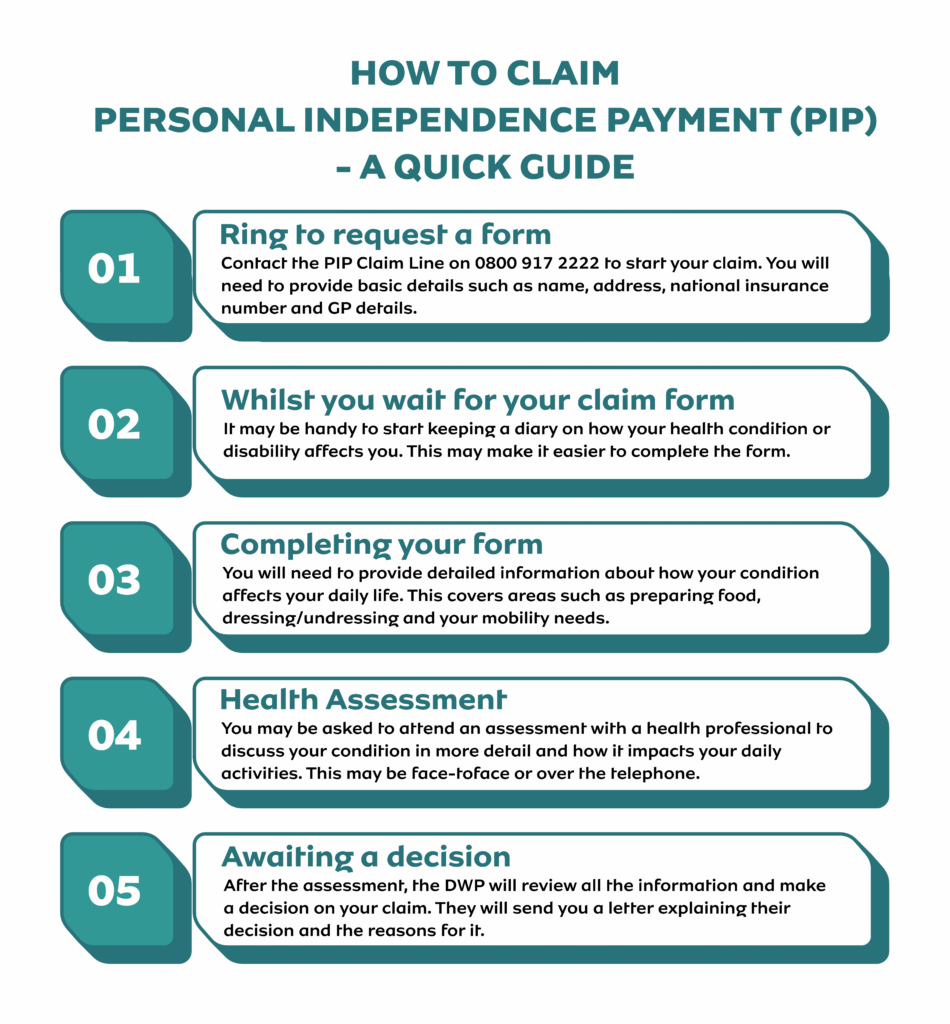
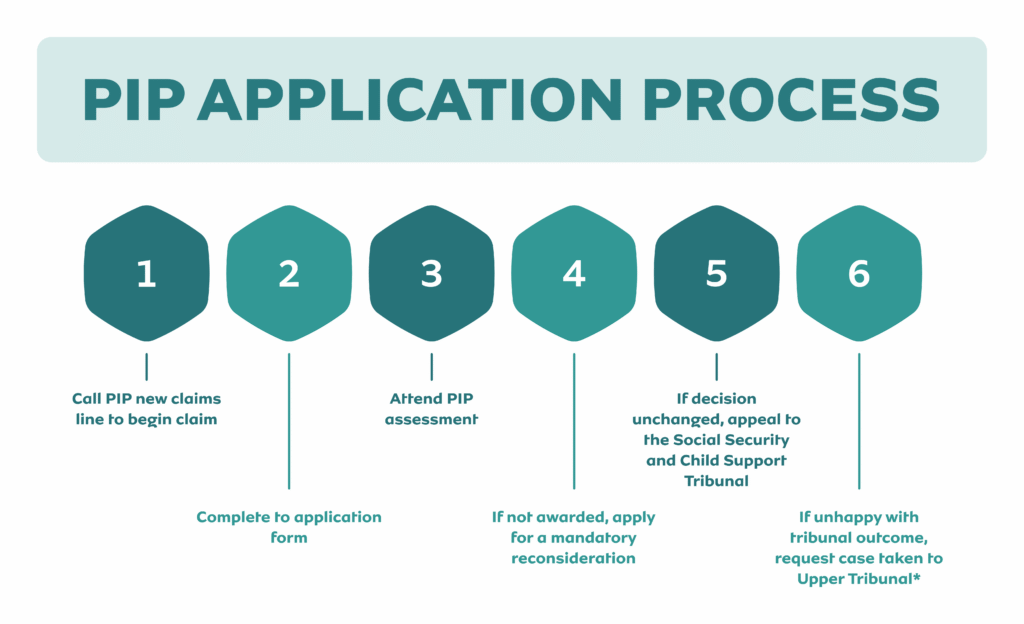
Step 1: Start Your Claim by Calling the DWP
You must begin the process by calling the pip contact number for new claims:
- New PIP claims: 0800 917 2222
- Opening hours: Monday to Friday, 8am–5pm
This dept work and pensions contact number allows the DWP to gather basic details before sending your application form.
During the call, the advisor will ask for:
- Your National Insurance number
- Your address and contact details
- Your bank account information
- Your GP or healthcare professional’s details
- Information about time spent in hospital or abroad
Many people search online for the number for personal independence payment or how do I contact DWP by phone, but the correct starting point for a new claim is the number above.
Once you complete the call, the DWP officially records the start date of your claim, which is important because PIP payments backdated usually begin from this date if your claim is successful.
Step 2: Complete the PIP Application Form
After your phone call, the DWP sends you the form called:
“How Your Disability Affects You” (PIP2).
Some people search for a PIP application form online, but the DWP normally sends this form by post after your initial call.
The form asks detailed questions about how your condition affects your ability to:
- Prepare meals
- Manage medication
- Wash and dress
- Communicate with others
- Travel and move around
Answer honestly and provide specific examples of difficulties you face. Caregivers often help complete this form because it requires clear explanations of daily challenges.
Step 3: Provide Supporting Evidence
Supporting documents strengthen your claim. Examples include:
- GP letters or specialist reports
- Prescription lists
- Care plans
- Statements from caregivers or family members
Evidence helps the DWP understand your needs before the assessment stage.
Step 4: Attend a PIP Assessment
Most people attend an assessment with a healthcare professional. This may happen:
- Face-to-face
- By telephone
- By video call
The assessor asks how your condition affects your everyday life. They then send a report to the DWP.
Step 5: Receive the Decision
After reviewing the assessment and evidence, the DWP sends a decision letter explaining:
- Whether you qualify for PIP
- Which component you receive
- Whether you receive the standard or enhanced rate
If the decision seems incorrect, you can challenge it through a process called mandatory reconsideration.
Many caregivers stay involved throughout the claim because they help explain how the person’s condition affects daily life and assist with contacting the pip enquiry line if problems arise.
How Much Is PIP Per Month? (2025/26 Payment Rates)
Many people ask “How much is PIP per month?” when deciding whether to apply. Personal Independence Payment is normally paid every four weeks, but the official rates are calculated weekly.
Your total payment depends on which components you qualify for and whether you receive the standard or enhanced rate.
Daily Living Component
You may receive this part if you need help with everyday activities such as preparing food, washing, dressing, managing medication, or communicating.
Current weekly rates (2025/26):
- Standard rate: £73.90 per week
- Enhanced rate: £110.40 per week
Approximate monthly payments:
- Standard rate: about £295 per month
- Enhanced rate: about £441 per month
Mobility Component
You may receive the mobility component if your condition affects how you move around or plan journeys.
Current weekly rates (2025/26):
- Standard rate: £29.20 per week
- Enhanced rate: £77.05 per week
Approximate monthly payments:
- Standard rate: about £117 per month
- Enhanced rate: about £308 per month
Maximum PIP Payment Per Month
If you qualify for the enhanced rate of both components, the maximum amount is approximately:
- £187.45 per week
- About £750 per month
Actual payments arrive every four weeks, so the amount deposited in your bank account may look slightly higher than a typical monthly payment.
Can PIP Payments Be Backdated?
Yes. In many cases, PIP payments backdated start from the date you first contacted the Department for Work and Pensions contact number to begin your claim.
For example, if the DWP takes several months to process your application, you may receive a lump-sum back payment covering the time between the start of your claim and the decision date.
Special Rules for Terminal Illness
People with a progressive illness and limited life expectancy may qualify under special rules. In these cases:
- The process moves faster
- The assessment may not be required
- The claimant usually receives the enhanced daily living rate automatically
Understanding how much PIP pays per month helps caregivers and families plan financially, especially when they rely on this support to manage the extra costs of disability or long-term illness.
SEE ALSO: What Is a Care Needs Assessment? (England Guide for Families and Caregivers)
What Other Benefits Can You Claim With PIP?
Many families ask “what other benefits can I claim with PIP?” because receiving Personal Independence Payment often unlocks additional financial support. PIP itself is not means-tested, but it can increase eligibility for other benefits and schemes that help cover daily living costs.
Understanding these options can make a significant difference for both claimants and caregivers.
Universal Credit
If you receive PIP, your Universal Credit award may increase. In many cases, you may qualify for the Limited Capability for Work and Work-Related Activity (LCWRA) element, which adds extra monthly support.
PIP can also help remove certain work requirements if your condition limits your ability to work.
Carer’s Allowance
If someone provides regular care for you, they may qualify for Carer’s Allowance.
A caregiver may claim this benefit if they:
- Provide at least 35 hours of care per week
- Care for someone receiving the daily living component of PIP
This support helps families who rely on caregivers to manage daily activities.
Housing Benefit or Universal Credit Housing Support
Receiving PIP can increase eligibility for:
- Housing Benefit
- Additional housing elements within Universal Credit
Local authorities often consider disability-related benefits when assessing housing support.
Council Tax Reduction
Many councils offer Council Tax discounts or reductions for households where someone receives PIP.
The exact amount depends on local council policies, but the reduction can significantly lower monthly bills.
Motability Scheme
If you receive the enhanced mobility component of PIP, you may qualify for the Motability Scheme.
This program allows you to lease:
- A car
- A wheelchair-accessible vehicle
- A mobility scooter
The payment comes directly from your mobility component.
Disabled Person’s Railcard and Travel Support
Some people who receive PIP may qualify for:
- Disabled Person’s Railcard
- Discounted public transport
- Local travel support programs
These benefits help reduce travel costs for medical appointments, work, and daily life.
Other Financial Support
Depending on your circumstances, PIP may also increase eligibility for:
- Disability-related grants
- Energy bill support programs
- Local authority assistance schemes
Because PIP confirms that a person has long-term disability-related needs, many support programs use it as proof when assessing eligibility.
Caregivers often help manage these applications and may contact the pip enquiry line or the dept work and pensions contact number if they need confirmation of an award letter.
MORE: What Is Respite Care in the UK? 2026
How to Contact the DWP About PIP Changes or Payment Issues
If your situation changes or you have problems with a payment, you should contact the Department for Work and Pensions (DWP) as soon as possible. Reporting PIP changes quickly helps prevent overpayments, payment delays, or interruptions to your claim.
The easiest way to do this is by calling the official PIP enquiry line.
PIP Contact Number for Existing Claims
If you already receive PIP or want to ask about your payments, use the pip contact number existing claim below:
- PIP enquiry line: 0800 121 4433
- Textphone / Relay UK: 0800 121 4493
- Opening hours: Monday–Friday, 9am–5pm
Many people search for the dwp contact number 0800, the dept work and pensions contact number, or the dept work and pensions tel no when trying to resolve issues with their claim. The number above connects you directly to the DWP team that handles Personal Independence Payment.
Reasons to Contact the PIP Enquiry Line
You should call the pip contact number 0800 if you need to report or discuss:
- PIP changes to your health condition
- A change of address or contact details
- A hospital stay or care home admission
- Problems with PIP payments
- Questions about your decision letter or award review
- Missing or delayed payments
Caregivers often call the dept of work and pensions contact no on behalf of family members who cannot manage the claim themselves.
What Information to Have Ready
Before calling the PIP enquiry line, prepare the following details:
- Your National Insurance number
- Your date of birth
- Your current address
- Details about the change you need to report
- Any letters you received from the DWP
Having this information ready helps the advisor locate your claim quickly and resolve the issue faster.
When the DWP May Ask You to Contact Someone Else
Sometimes the Department for Work and Pensions contact number cannot resolve your issue directly.
For example, if your question relates to a medical assessment appointment, the DWP may ask you to contact the company handling the assessment instead. These providers may include:
- Capita
- Ingeus
- Maximus
They manage assessment appointments and reports used to determine your PIP award.
Scotland Update: PIP and Adult Disability Payment (ADP)
If you live in Scotland, the system has changed. The Scottish Government has gradually replaced Personal Independence Payment (PIP) with a new benefit called Adult Disability Payment (ADP). This transition forms part of the wider Scotland PIP ADP update, which moved disability benefits from the Department for Work and Pensions to Social Security Scotland.
What Is Adult Disability Payment (ADP)?
Adult Disability Payment provides similar support to PIP for people with long-term disabilities or health conditions. It still includes two components:
- Daily living support
- Mobility support
Like PIP, the payment helps people cover the extra costs of living with a disability or long-term health condition.
Who Should Apply for ADP Instead of PIP?
If you live in Scotland and need to make a new claim, you usually apply for Adult Disability Payment, not PIP.
You may still receive PIP if:
- You claimed PIP before ADP replaced it, or
- Your claim is still being transferred to Social Security Scotland
The government is gradually moving existing PIP claimants in Scotland to ADP through a managed transfer process. During this transition, most people continue receiving payments without needing to reapply.
What Happens If You Move Between Scotland and England or Wales?
Your benefit may change depending on where you live.
- If you move from Scotland to England or Wales, you may need to apply for PIP again through the Department for Work and Pensions contact number.
- If you move from England or Wales to Scotland, your PIP claim may eventually transfer to Adult Disability Payment.
It is important to report these changes to the relevant authority so your payments continue without interruption.
Contacting the Correct Department
People sometimes search online for the pip contact number or the dept work and pensions contact number even though they now receive ADP.
If you live in Scotland and receive ADP, you should normally contact Social Security Scotland instead of the DWP.
Understanding the Scotland PIP ADP update helps avoid confusion and ensures you contact the correct department when you need help with your disability benefits.
ALSO READ: Is MS Hereditary or Inherited? What Causes Multiple Sclerosis (2026)
When to Contact the Assessment Provider Instead of the DWP
In some situations, calling the PIP enquiry line or the Department for Work and Pensions contact number will not resolve your issue. This usually happens when your question relates to the medical assessment used to decide your claim.
The DWP reviews the final decision, but a separate organisation normally carries out the assessment itself.
Assessment Providers Used for PIP
Depending on where you live, the assessment may be handled by one of the following providers:
- Capita
- Ingeus
- Maximus
These organisations arrange and conduct the health assessments that help determine whether you qualify for Personal Independence Payment.
When You Should Contact the Assessment Provider
You may need to contact the assessment provider directly if you need to:
- Reschedule an assessment appointment
- Ask about the location or format of your assessment
- Request reasonable adjustments for a disability
- Check whether your medical evidence was received
- Confirm details of a telephone or video assessment
If you try to resolve these issues through the pip contact number, the DWP will usually refer you back to the assessment provider because they manage the appointment process.
Preparing for Your Assessment
Your assessment gives you an opportunity to explain how your condition affects your daily life. Preparing in advance can help you communicate your situation clearly.
Consider bringing or preparing:
- Medical reports from your GP or specialist
- Prescription lists or treatment plans
- A daily routine diary describing your difficulties
- Statements from caregivers or family members
Caregivers often attend the assessment or help explain the challenges the claimant faces each day.
What Happens After the Assessment
After the assessment, the healthcare professional sends a report to the Department for Work and Pensions. The DWP then reviews the report and your evidence before making the final decision on your PIP claim.
If you disagree with the decision, you can request a mandatory reconsideration, which allows the DWP to review your case again.
Tips for Caregivers Calling the PIP Enquiry Line
Many people who contact the PIP enquiry line do so on behalf of a family member. Caregivers often manage the claim, report PIP changes, and resolve payment issues for someone who cannot handle the process alone.
Calling the Department for Work and Pensions contact number can sometimes take time, so preparing in advance will make the conversation easier and faster.
Call at the Right Time
The pip contact number 0800 can experience long waiting times, especially during busy periods.
To reduce delays:
- Call early in the morning
- Avoid Monday mornings, when call volumes are highest
- Expect waiting times to sometimes exceed 30–60 minutes
Planning your call can help you reach an advisor sooner.
Have Important Information Ready
Before calling the dept work and pensions contact number, make sure you have the key details ready. This helps the advisor locate the claim quickly.
Prepare:
- The claimant’s National Insurance number
- Full name and date of birth
- Address linked to the claim
- Any letters received from the DWP
- Details of the issue or change you want to report
Caregivers should also explain that they are calling on behalf of the claimant, as the advisor may need to confirm permission before discussing the claim.
Clearly Explain the Reason for Your Call
When speaking to the advisor, explain the issue clearly. Common reasons for contacting the pip enquiry line include:
- Reporting PIP changes to health conditions
- Asking about missing or delayed payments
- Checking the progress of a claim or review
- Updating contact or bank details
Providing clear information helps the advisor resolve the issue more quickly.
Take Notes During the Call
Write down important details during the conversation, such as:
- The date and time of the call
- The name of the advisor
- Any reference numbers or instructions
Keeping records can help if you need to follow up with the Department for Work and Pensions contact number later.
Consider Alternative Support
If you struggle to manage the claim process, organisations such as Citizens Advice or local disability support services can offer guidance on dealing with the DWP and managing PIP claims.
Caregivers who understand how the pip enquiry line works often find it much easier to support a loved one through the application, review, and payment stages.
Final Thoughts…
Understanding Personal Independence Payment (PIP) can feel overwhelming, especially for caregivers who manage claims for a loved one. The process involves checking Personal Independence Payment eligibility, contacting the Department for Work and Pensions, completing the PIP application form, and attending an assessment before receiving a decision.
If you need help with an existing claim, the PIP enquiry line remains the fastest way to speak directly with the DWP. The main pip contact number for existing claims is 0800 121 4433, which connects you to the Department for Work and Pensions contact number for payment questions, claim updates, or reporting PIP changes.
For new claims, you can start the process by calling 0800 917 2222, where an advisor will guide you through the first steps of how to apply Personal Independence Payment.
Many caregivers also want to understand how much PIP pays per month, whether PIP payments can be backdated, and what other benefits can be claimed with PIP. Knowing these details can help families plan financially and ensure the claimant receives the full support available.
If you live in Scotland, remember that the Scotland PIP ADP update means many new claims now fall under Adult Disability Payment, which Social Security Scotland manages instead of the DWP.
Although the process may seem complex at first, thousands of people successfully claim PIP each year with the help of caregivers, healthcare professionals, and support organisations. Preparing the right information, understanding the eligibility rules, and contacting the correct dept work and pensions contact number when needed can make the process much smoother.
For many families, PIP provides essential financial support that helps cover the additional costs of living with a disability or long-term health condition.
Need Help Understanding PIP or Supporting Someone With a Claim?
If you are supporting someone with a disability and feel unsure about Personal Independence Payment eligibility, the PIP application process, or how to deal with the Department for Work and Pensions, Care Sync Experts can help.
We support caregivers and families by explaining PIP rules in plain language, helping you understand what evidence is needed, how the assessment process works, and what steps to take if a claim becomes delayed or a decision seems incorrect.
Our team helps you avoid common mistakes that often lead to delayed payments, failed assessments, or unnecessary stress, so you can focus on supporting the person who needs care.
Whether you are preparing to apply for PIP, managing an existing claim, or trying to understand the support and benefits available, we are here to guide you through the process with clarity and confidence.
FAQ
How long does PIP last?
Personal Independence Payment (PIP) usually lasts for a fixed award period decided by the Department for Work and Pensions (DWP). Many people receive an award that lasts between 1 and 10 years, depending on how their condition affects them and whether their situation may change over time.
Before the award ends, the DWP normally reviews the claim. They may ask you to complete a review form or attend another assessment to confirm whether you still qualify for PIP and whether the payment rate should stay the same.
Some people with long-term or lifelong conditions receive ongoing awards, which do not have a set end date but are still reviewed periodically.
Can I claim PIP if I work?
Yes, you can claim Personal Independence Payment even if you work. PIP focuses on how your health condition or disability affects your daily living and mobility, not your employment status.
This means you may qualify for PIP if you:
– Work full time
– Work part time
– Are self-employed
The Department for Work and Pensions assesses the difficulty you have completing daily activities, rather than whether you earn a salary. Many people continue working while receiving PIP because the payment helps cover the extra costs associated with disability or long-term health conditions.
What documents are needed to apply for PIP?
When applying for Personal Independence Payment, you should provide supporting evidence that explains how your condition affects your daily life. Strong evidence can help the DWP understand your needs before your assessment.
Common documents include:
– Letters or reports from your GP or medical specialist
– Prescription records or medication lists
– A care plan or treatment plan
– Statements from caregivers, family members, or support workers
– A daily routine diary explaining your difficulties
Providing clear evidence makes it easier for the assessor to understand how your condition affects everyday activities such as washing, dressing, cooking, or travelling.
How is PIP back paid?
If your claim is successful, the Department for Work and Pensions may issue backdated PIP payments. This means you receive a lump sum covering the period between the date you started your claim and the date the decision was made.
For example, if you started your claim in January but the DWP approved it in April, you could receive several months of back payments in your first deposit.
These payments usually arrive as a single lump sum, followed by regular PIP payments every four weeks going forward.