The Children’s Homes (England) Regulations 2015 set the main legal rules for registered children’s homes in England. They require providers to deliver safe, child-centred care through nine Quality Standards and to meet wider duties around leadership, staffing, safeguarding, monitoring and Ofsted registration.
For providers, the children’s home regulations should guide everyday decisions, not sit unused in a policy folder. They shape how staff listen to children, plan care, manage risks, support education, build relationships and respond when concerns arise.
The regulations apply to homes that provide care and accommodation for children and young people. They aim to make sure every child lives in a home that supports their safety, wellbeing, development and individual goals.
This guide explains what are the children’s home regulations 2015, what they mean for care providers, and how managers can turn legal requirements into safer, more consistent care.
Why the Regulations Matter to Children’s Home Providers
Children’s care home regulations give providers a clear framework for running a home that protects children and helps them make progress. They set expectations for how leaders recruit staff, plan care, manage risks, support education, respond to safeguarding concerns and review the quality of the service.
For caregivers, the regulations turn broad values such as dignity, safety and respect into daily actions. Staff should know each child’s needs, listen to their views, follow care plans, record concerns clearly and act quickly when something changes.
Strong compliance also helps providers create a more stable home. When managers set clear standards, supervise staff well and review incidents properly, they reduce avoidable risks and build a safer environment for children and colleagues.
The regulations are not only about passing an Ofsted inspection. They help providers deliver the kind of care that gives children consistency, positive relationships and a real chance to thrive.
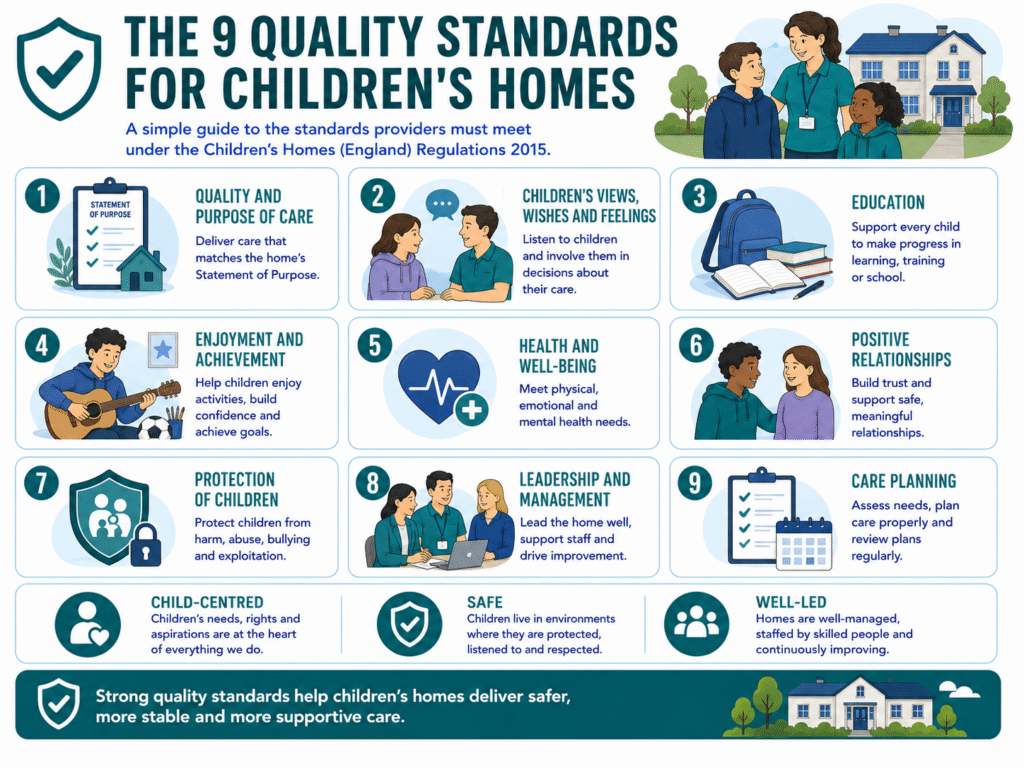
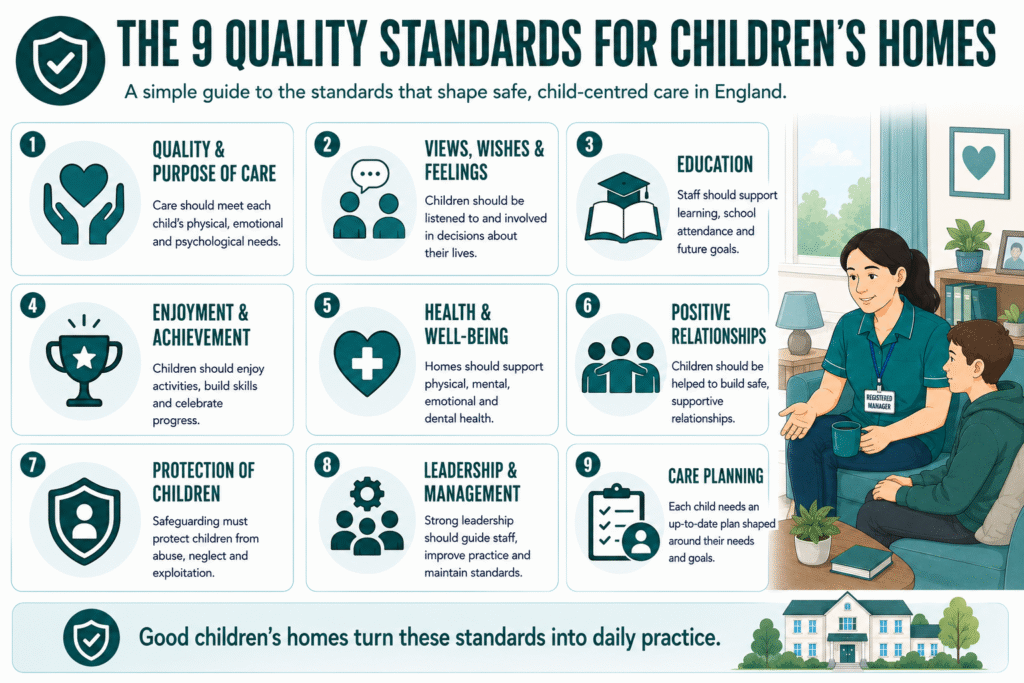
The 9 Quality Standards: What They Mean in Daily Practice
The list of children’s homes regulations includes nine Quality Standards. Together, they help providers create a safe, stable and supportive home where children can feel heard, make progress and build confidence.
| Quality Standard | What It Means in Practice |
| Quality and purpose of care | The home must provide care that matches each child’s physical, emotional and psychological needs. Managers should make sure the Statement of Purpose accurately reflects the children the home supports. |
| Children’s views, wishes and feelings | Staff should involve children in decisions about their routines, care plans, goals and home life. Children need clear ways to raise concerns and know adults will listen. |
| Education | Staff should actively support school attendance, learning, homework, training and future goals. They should work closely with schools, virtual schools and placing authorities. |
| Enjoyment and achievement | Children should have opportunities to enjoy hobbies, social activities, celebrations, life skills and achievements that build confidence. |
| Health and well-being | The home must support physical, emotional, mental and dental health. This includes appointments, healthy routines, medication support and access to specialist help where needed. |
| Positive relationships | Staff should help children build safe relationships with family, friends, professionals and peers. They should also model calm, respectful communication. |
| Protection of children | Providers must apply strong safeguarding principles, identify risks early and respond quickly to concerns such as abuse, exploitation, missing episodes or harmful behaviour. |
| Leadership and management | Leaders must guide staff well, monitor care quality, provide supervision and make sure the workforce has the skills to meet children’s needs. |
| Care planning | Every child needs an up-to-date plan that explains their needs, goals, risks, routines and support network. Staff should use it actively, not treat it as paperwork. |
Childrens home regulations health and safety should run through every standard. For example, a safe home does not only have secure premises and clear risk assessments. It also creates predictable routines, strong relationships, good communication and prompt action when a child’s needs change.
RELATED: Children’s DLA Rates: Who Qualifies, and What to Claim in 2026
Safeguarding: What Providers Must Get Right
Safeguarding must shape every part of life in a children’s home. Providers need clear procedures, but staff also need the confidence to spot concerns early, record them properly and escalate them without delay.
A strong safeguarding approach should include safer recruitment, DBS checks, regular training, clear reporting routes and consistent supervision. Staff should understand how to respond to missing episodes, allegations, exploitation risks, self-harm concerns, bullying, unsafe relationships and changes in behaviour.
The principles of safeguarding require staff to act in the child’s best interests, listen carefully, share concerns with the right professionals and avoid waiting for a situation to worsen. A child protection plan may set out specific actions for a child at risk, while Section 47 of the Children’s Act 1989 gives local authorities a duty to make enquiries where they suspect significant harm.
Providers should also understand the wider Children’s Act 1989 framework. Section 17 focuses on children in need, while Section 47 focuses on children who may be suffering or likely to suffer significant harm. These duties sit alongside the home’s own responsibility to protect every child in its care.
Leadership, Staffing and Qualifications
Strong leadership turns children’s home regulations into consistent daily care. The registered manager should lead the home closely, support staff, review concerns and make sure every child receives care that matches their needs.
Providers also need a responsible individual when an organisation runs the home. This person should oversee the service at a higher level, challenge poor practice and make sure the provider meets its legal duties.
Children’s home regulations qualifications do not mean every team member needs the same certificate. However, providers must employ people with the right skills, experience and training for the children they support. This may include trauma-informed care, behaviour support, safeguarding, mental health awareness, medication, autism, learning disabilities or exploitation risks.
A good staffing plan should also cover supervision, induction, rota gaps, sickness, recruitment and emergency cover. Children need familiar, capable adults around them, especially when they have experienced instability or trauma.
In children’s home regulations 2026, providers should focus on more than filling shifts. They should build a stable workforce that understands each child, works consistently and responds calmly when needs change.
READ MORE: Supported Accommodation Regulations: 2026 Practical Ofsted Compliance Guide
The Documents and Reviews That Keep a Home Compliant
Good children’s homes use documents as working tools, not paperwork for inspection day. The Statement of Purpose should clearly explain who the home supports, the care it provides and how staff will meet children’s needs. Managers should review it whenever the service changes.
Each child also needs an up-to-date care plan, risk assessment and placement information. These records should reflect the child’s wishes, health needs, education, family relationships and any safeguarding concerns. Staff should update them when a child’s needs, behaviour or circumstances change.
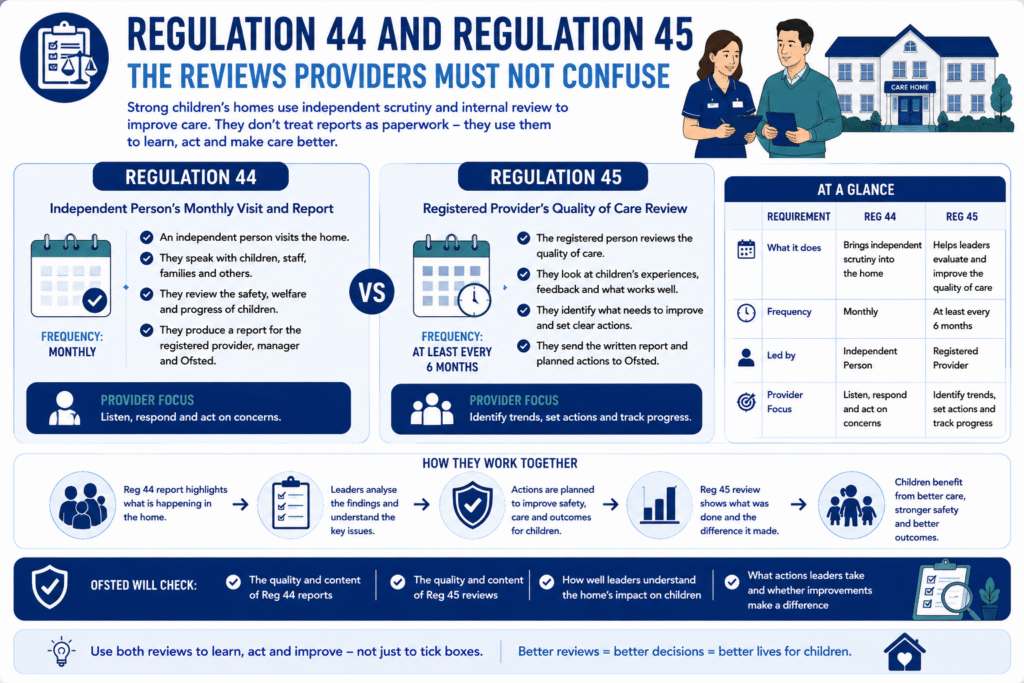
Providers must also monitor the quality of care. Regulation 44 requires an independent person to visit the home every month and report on children’s safeguarding, wellbeing and lived experience. Regulation 45 requires providers to review the quality of care at least every six months and identify improvements.
Managers should use these reviews to spot patterns, challenge weak practice and improve care before issues become more serious. They should also work appropriately with people who hold parental responsibility, placing authorities and other professionals involved in each child’s care.
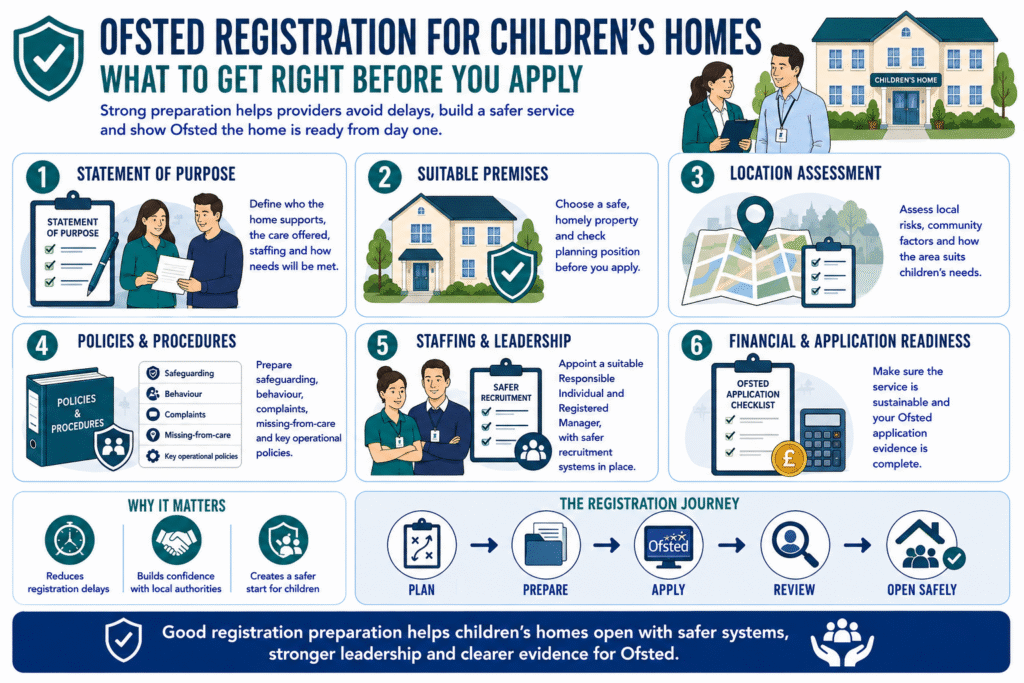
What Ofsted Will Expect During Registration and Inspection
Ofsted expects providers to show that they can run a safe, stable and child-centred home from day one. Your home should match its Statement of Purpose, support the children you say you will care for and have enough suitably skilled staff in place.
During registration and inspection, Ofsted will look closely at how children experience the home. Inspectors will want to see that staff understand each child’s needs, manage risks properly, support education and health, and build trusting relationships.
Providers should also be ready to explain:
- why the property is suitable for the children they plan to support
- how the location promotes safety, community access and positive opportunities
- how staffing levels and training match children’s needs
- how leaders respond to incidents, complaints and safeguarding concerns
- how the home avoids unnecessary restrictions and supports children to live as normally as possible
A well-prepared home does not wait for an inspection to improve. It reviews practice regularly, listens to children and acts quickly when standards slip.
SEE ALSO: What is Regulated Activity? 2026 DBS Update, Examples
Children’s Home Compliance Checklist for Providers
Use this quick checklist to review whether your home is meeting the key children’s home regulations in daily practice:
- Our Statement of Purpose matches the children we support.
- Our staffing levels, rotas and training meet children’s needs.
- Staff understand safeguarding principles and know how to report concerns.
- Children can share their views, wishes and worries safely.
- Care plans and risk assessments stay current and child-centred.
- We support education, health, relationships and personal development.
- We complete Regulation 44 visits and act on the findings.
- We complete Regulation 45 reviews and track improvements.
- Managers review incidents, complaints, missing episodes and safeguarding trends.
- We prepare for Ofsted every day through good care, not last-minute paperwork.
The strongest providers use this checklist as a routine management tool. It helps managers identify gaps early, support staff properly and keep the home focused on children’s safety, wellbeing and progress.
Regulations Should Improve Children’s Lives
Children’s home regulations should do more than help providers meet Ofsted requirements. When leaders apply them well, they create homes where children feel safe, listened to and supported to build a better future.
The best providers turn legal duties into everyday habits: staff know each child well, managers respond quickly to concerns, and children have a real say in their lives.
Care Sync Experts supports children’s home providers with registration preparation, policy development, compliance audits, staff training and Ofsted readiness.
FAQ
What is Regulation 26 of the Children’s Homes (England) Regulations 2015?
Regulation 26 covers the fitness of the registered provider. It requires the provider to be a person of integrity and good character, with the skills, experience and financial capacity needed to run a children’s home safely and effectively.
Where the provider is an organisation, Ofsted will also expect it to appoint a suitable responsible individual who can represent the provider and oversee the home.
What is Regulation 32 of the Children’s Homes (England) Regulations 2015?
Regulation 32 covers staff recruitment and employment checks. Providers must use recruitment procedures that protect children’s safety and must have the required information about each staff member before allowing them to work in the home.
This includes identity checks, references, employment history, qualifications where relevant, and DBS-related safeguarding checks set out in Schedule 2. Providers should also investigate gaps, inconsistencies or concerns before appointing someone.
What is Regulation 43 of the Children’s Homes (England) Regulations 2015?
Regulation 43 requires the registered provider to appoint an independent person to visit the children’s home and prepare a report on the home’s safeguarding arrangements and the quality of care provided.
The independent person should speak with children, staff and other relevant people where appropriate, review records and identify whether the home protects and promotes children’s welfare. The provider must then consider the report and act on any concerns or recommendations.
What is Regulation 40 of the Children’s Homes (England) Regulations 2015?
Regulation 40 covers notifications of serious events. The registered person must notify Ofsted and other relevant bodies when certain serious incidents occur, such as the death of a child, a serious injury, allegations of abuse, police involvement, a child going missing in serious circumstances, or other significant safeguarding events.
Providers should have a clear notification process so staff report incidents promptly, managers assess the event correctly, and the home meets its legal reporting duties without delay.